*Last updated 5/26/26
Hormone Replacement Therapy (HRT) is a valid treatment option for women who are transitioning from perimenopause to menopause. Surrounded in controversy over the years, this treatment is not wholly natural & holistic, but there are options that minimize the artificiality. If your symptoms include: hot flashes, poor sleep, sexual challenges and mood swings, HRT does offer improvement with limited side effects, so long as your personal health history and timing to menopause is appropriate.
This article will help you decide whether you or your clients are candidates for HRT.

What Happens from Perimenopause to Menopause
Perimenopause and menopause represent one of the most significant hormonal transitions in a woman’s life.
The transition from reproductive to nonreproductive function is known as perimenopause. It typically begins years before the final menstrual period, when ovarian hormone production becomes irregular. Perimenopause typically lasts 4–7 years but extends up to 10–14 years in some women.[1] Since the average age of menopause in the U.S. is 51–52,[2] perimenopause may begin as early as the late 30s to early 40s.
During perimenopause:
- Ovarian hormone function becomes erratic.
- Estrogen and progesterone have irregular fluctuations in timing and magnitude that contribute to variable and often confusing symptoms.[3,4,5]
- Menstrual cycles become irregular.
Eventually menopause occurs, defined medically as 12 consecutive months without a menstrual period.
At that point:
- Progesterone production essentially stops.[6]
- Estrogen production drops dramatically.[7]
Menopause therefore represents more than the end of menstruation. It is a system-wide endocrine shift caused by the loss of ovarian hormone production.
These hormones influence many physiological systems, including:
- bone metabolism
- brain signaling
- vascular function
- body-fat distribution
- collagen integrity
The decline of these hormones is responsible for many of the symptoms women experience during this stage of life.
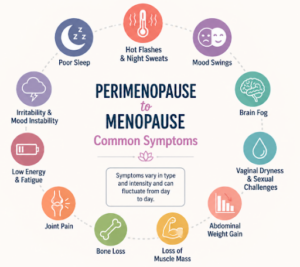
Common symptoms include:
- hot flashes and night sweats (these are referred to as Vasomotor Symptoms, VMS)
- sleep disturbance
- mood instability
- brain fog
- vaginal dryness
- loss of libido
- bone loss
- increased abdominal fat
- loss of muscle mass
- joint pain
Two Philosophies About Menopause
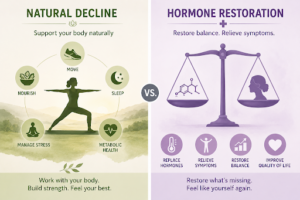
There are two main philosophical approaches to menopause management, natural decline or hormone restoration.
1. Natural Decline
The natural decline perspective views menopause as a natural life transition that does not necessarily require medical treatment.
In this approach, the focus is on supporting overall health through lifestyle strategies such as:
- exercise
- nutrition
- sleep
- stress management
- metabolic health
Many women can manage symptoms effectively with these foundational strategies, able to thrive and feel strong, capable, and fully engaged in daily life.
2. Hormone Restoration
The hormone restoration perspective views menopause as a medical condition – hormone deficiency – requiring intervention, similar to other endocrine changes in medicine. From this viewpoint, replacing hormones may restore physiological balance and improve quality of life.
Many women report that HRT is a life-transforming decision that significantly improves their quality of life, often restoring their ability to function, work, and feel like themselves again.
Foundational Health Still Matters
Before discussing hormone therapy, it is important to emphasize that wellness remains foundational.
For women navigating perimenopause and menopause, core health pillars still play the primary role in long-term health outcomes.
KEY for Various Types of Scientific Research
- REVIEW – Scientific Review is a paper that summarizes and interprets findings from multiple existing studies on a topic.
- RCT – Randomized Control Trial is a study in which participants are randomly assigned to an intervention or control group to test cause-and-effect relationships.
- CSS – Cross Sectional Study looks at a group of people at one single point in time to examine relationships between variables.

Breathing
- Thomas. Rajiv Gandhi University of Health Sciences (India).[8]
- In a pre-experimental study (no control group) of 60 menopausal women, deep breathing exercises significantly reduced hot-flush severity, with mean scores decreasing from 31.95 pre-intervention to 12.69 post-intervention, indicating a substantial improvement in symptom burden.
- Conclusion: “The present study attempted to assess the effectiveness of deep breathing exercise in relieving of hot flush among menopausal women and found that the deep breathing exercise was effective in relieving the hot flush of menopausal women.”
- Iyyappan. TNNMC Journal of Obstetrics and Gynaecological Nursing.[9] RCT
- In a study of 40 menopausal women, participants in the experimental https://www.wbs-ulm.de/ group who practiced deep breathing showed substantially lower post-test symptom scores (mean 8.25) compared with the control group using routine home remedies (mean 25.45), with a statistically significant difference (t = 13.54, P < 0.0001).
- Conclusion: “The study concluded that the deep breathing exercise had significant effect in reduction of menopausal symptoms among menopausal women.”

Exercise
- Sternfeld, et al. The Journal of The Menopause Society.[10] AEROBIC EXERCISE RCT
- In a randomized controlled trial of 248 late perimenopausal and postmenopausal sedentary women with frequent vasomotor symptoms, a 12-week aerobic exercise program did not significantly reduce vasomotor symptom frequency or bother compared with usual activity, although small improvements were observed in sleep quality and depressive symptoms.
- Conclusion: “These findings provide strong evidence that 12 weeks of moderate-intensity aerobic exercise do not alleviate VMS but may result in small improvements in sleep quality, insomnia, and depression in midlife sedentary women.”
- Nguyen et al. IJERPH[11] YOGA & PELVIC FLOOR EXERCISE REVIEW
- In a systematic review and meta-analysis of 9 randomized controlled trials involving 882 women with menopausal symptoms, exercise showed positive effects on physical and psychological quality-of-life scores, but there was no clear evidence of benefit for general, social, or menopause-specific quality-of-life measures.
- Types of exercise:
- Pelvic Floor (3)
- Yoga (4)
- Aerobic (1)
- Walking (1)
- Types of exercise:
- Conclusion: “This systematic review found positive effects of exercise on physical and psychological QoL scores in women with menopausal symptoms. However, there were no evident effects of exercise on…menopause-specific QoL scores in women after exercise interventions compared with no active interventions.”
- Berin et al. BMC.[12] STRENGTH TRAINING RCT
- In a qualitative study of 15 low-active postmenopausal women who completed a 15-week resistance-training program, participants reported that hopes of relieving vasomotor symptoms initially motivated them to begin training, while ongoing accountability, professional support, and improving well-being helped sustain adherence; most women also reported improvements in vasomotor symptoms and all had increased their physical activity one year later.
- Conclusion: “Resistance training improved general well-being and most women experienced improvement in VMS.”
- VMS – Vasomotor symptoms, including hot flashes & night sweats.
- Berin, et al. Climacteric.[13] STRENGTH TRAINING RCT
- In this trial of 65 postmenopausal women with daily vasomotor symptoms, 15 weeks of resistance training (3×/week) significantly improved menopause-specific quality-of-life domains including vasomotor symptoms, sleep problems, and menstrual symptoms, compared with an untreated control group. No significant differences were found in general health-related quality-of-life summary scores
- Conclusion: “In postmenopausal women with moderate to severe VMS, resistance training three times per week for 15 weeks improved menopause-specific HRQoL.”
- Capel-Alcaraz, et al. Journal of Clinical Medicine.[14] STRENGTH TRAINING REVIEW
- This systematic review of 12 randomized trials found that strength (resistance) exercise in menopausal women improved muscle strength, physical activity levels, bone density, and certain hormonal and metabolic markers. These improvements may contribute to better physical functioning related to quality of life. However, evidence for consistent improvements in menopausal symptoms and overall quality-of-life measures was mixed, partly due to heterogeneity in exercise protocols.
- Conclusion: “Considering the studies encountered, strength exercises can be beneficial for improving menopausal symptoms that affect muscle performance in general, physical activity, bone density and hormonal and metabolic responses such as heart rate, blood pressure and hot flashes. In terms of the appropriate type of strength training, the evidence is still unclear given that the same benefits are achieved by various types of exercises and with various accessory methods.”

Nutrition quality, including protein intake
- Erdélyi. Nutrition and Hormone Regulation.[15] REVIEW
- This review found that dietary counseling and balanced nutrition during perimenopause and menopause may help reduce disease risk and symptom burden by improving weight status, metabolic health, cardiovascular risk, bone health, and key nutrient intake, with particular emphasis on protein, calcium, vitamin D, vitamin C, B vitamins, fiber, and healthy fats.
- Conclusion: “Following the guidelines of a balanced diet reduces symptoms and preserves health.” This statement precedes a list of 21 specific items that identify what these authors consider to be important nutritional habits, including things like: avoiding sugar, eating enough protein, adequate vitamins, and more.
- Yang. Nutrients.[16] CSS – a “snapshot” analyzing data from one point in time.
- In a large cross-sectional study of 52,347 women aged 35–60 years, higher intake of fish, milk, and soy products was significantly associated with reduced severity of menopausal symptoms, and greater fish consumption showed a dose-response relationship with delayed natural menopause, whereas calcium and iron supplement use was associated with increased symptom severity.
- Conclusion: “The intake of fish, milk, and soy products plays a role in alleviating the severity of menopausal symptoms, particularly in delaying natural menopause, with the effect of fish intake being especially significant.”
- “The intake of fish, milk, and soy products was significantly negatively correlated with the severity of menopausal symptoms.”

Sleep health
Direct menopause-specific research on sunlight exposure or bedroom darkness for improving sleep is limited, but broader circadian science and a small amount of menopause-related light research suggest that light timing likely matters.
- Tal. Current Psychiatry Reviews.[17] (Menopause-specific)
- Practical environmental and lifestyle adjustments are recommended to improve sleep quality during menopause.
- “Sleep hygiene consists of recommending a variety of behaviors and tending to environmental factors (e.g., light, bedroom temperature) that are conducive to sleep and may decrease discomfort related to nocturnal hot flashes.”
- “Examples of sleep hygiene instructions include wearing lighter pajamas to bed… using lighter bedding and layering, keeping the ambient room temperature cool… limiting caffeine… avoiding alcohol and smoking, and obtaining exercise away from bedtime (> 4 hours).”
- Xu. Chronobiology International.[18] (Menopause-specific)
- This observational study found that in menopausal shift workers (11 shift and 38 day-workers), greater daily sunlight exposure was associated with reduced hot-flush severity, suggesting circadian-light exposure may influence vasomotor symptoms.
- Conclusion: “For shift workers, an hour increase in sunlight exposure was associated with a 1.4-point reduction in hot flush score… The finding of this study suggests increased sunlight exposure might improve hot flushes in menopausal shift workers who are moderately bothered by hot flushes, but probably not in day workers.”
- Menezes-Júnior. BMC Public Health.[19] CSS (general population)
- In a cross-sectional study of 1,762 Brazilian adults, greater morning sunlight exposure was associated with an earlier sleep midpoint and better overall sleep quality, while sunlight exposure was not significantly associated with total sleep time, sleep latency, or sleep efficiency. For every 30-minute increase in morning sunlight exposure before 10 a.m., the sleep midpoint was 23 minutes earlier, and the PSQI total score was modestly lower. (PSQI – Pittsburgh Sleep Quality Index.)
- Conclusion: “Morning sunlight exposure influences the regulation of the sleep midpoint and overall sleep quality. These findings highlight the potential role of morning sun exposure in aligning circadian rhythms and improving sleep health.”

Stress reduction and mind awareness
- Stefanopoulou. Grunfeld. Journal of Psychosomatic Obstetrics & Gynecology. SYSTEMATIC REVIEW[20]
- This systematic review evaluated 26 randomized controlled trials on mind–body therapies for menopausal vasomotor symptoms, finding consistent evidence supporting cognitive behavioural therapy (CBT) and relaxation techniques, while evidence for other interventions such as yoga, mindfulness, and paced breathing was mixed and limited by methodological variability.
- Conclusion: “Collectively, findings suggest that interventions that include breathing and relaxation techniques, as well as CBT, can be beneficial for alleviating vasomotor symptoms.”
- Thomas et al. Journal of Clinical & Diagnostic Research. REVIEW.[21]
- This review examined existing literature on mindfulness-based and other mind–body practices for menopausal symptom management. Findings suggest that mindfulness practices may help reduce psychological symptoms such as anxiety, irritability, and depression, and may improve sleep and overall wellbeing, although they may not significantly reduce vasomotor symptoms such as hot flashes.
- Conclusion: “Several researchers have discovered that being mindful may be helpful for menopausal women struggling with irritability, anxiety, and depression.”
—————————————-
Natural lifestyle factors influence metabolic health, inflammation, body composition, and hormonal signaling.
Hormone therapy should therefore be understood as a potential tool — not a replacement for foundational health behaviors.
HRT is Another Potential Solution
Hormone Replacement Therapy refers to the medical use of hormones to replace declining internal production. In general, “HRT can provide effective relief for a wide range of health conditions, potentially avoiding the need for multiple treatments for separate problems.”
In women, HRT usually involves:
- estrogen
- progesterone (if the uterus is present)
These hormones can be delivered through several methods, including:
- patches
- gels
- vaginal creams
- oral tablets
- hormonal ring insertion
Transdermal (patches, creams, gels) estrogen is often preferred in modern clinical practice because it bypasses liver metabolism and appears to carry a lower clotting risk than oral estrogen.[23]
Why Progesterone Is Needed When the Uterus Is Present
Estrogen stimulates growth in the lining of the uterus. It binds to receptors all over the body, including in the endometrium where it stimulates cell division, tissue thickening, and increased blood vessel growth.[24] This occurs just as it would every month in preparation for ovulation and potential pregnancy.
Progesterone acts as a regulatory signal that limits this growth. Progesterone slows endometrial cell proliferation, reduces estrogen receptor activity, promotes cellular differentiation, and encourages normal cell turnover.
Without progesterone, estrogen can continuously stimulate the uterine lining, increasing the risk of endometrial hyperplasia and cancer.
For this reason, women who still have a uterus generally require both hormones.
Bioidentical Hormones
Many modern HRT regimens use bioidentical hormones, meaning the hormone molecules are chemically identical to those produced by the body.
Common examples include:
- estradiol (bioidentical estrogen)
- micronized progesterone (bioidentical progesterone)
Bioidentical chemistry essentially binds to corresponding receptors in a similar physiologic manner as natural chemistry.
However, even bioidentical hormones do not perfectly recreate natural physiology.[25] For example, hormones produced by the ovaries follow complex pulsatile cycles,[26] at times for example, every 60-90 minutes.[27] In contrast, HRT is generally delivered in scheduled regimens – often steady transdermal estradiol with continuous combined progesterone rather than true physiologic pulsatility.[28]

Why “Bioidentical” Does Not Mean Identical Outcomes
A useful analogy comes from nutrition science.
Individual amino acids are chemically identical regardless of food source. For example, leucine from beef and leucine from lentils are molecularly identical.
However, the biological effects of those foods differ because of the surrounding nutritional matrix — including other amino acids, fiber, micronutrients, and digestion rates.
Hormones behave similarly.
Even when the molecule is identical, outcomes can vary depending on factors such as:
- dose
- delivery method
- receptor density in tissues
- metabolic health
- timing relative to menopause
- interactions with other hormones
Biology is not just chemistry. It’s signaling networks.
Compounded Bioidentical Hormones: Greater Complexity and Less Standardization
Compounded bioidentical hormones introduce additional complexity for individuals seeking the most pure therapeutic options. These formulations are custom-mixed by a compounding pharmacy, rather than standardized pharmaceutical manufacturing.
Although they may be marketed as “bioidentical,” these compounded products are not FDA-approved at the formulation level and are not subject to the same regulatory standards. Essentially, these compounded formulations can be a blessing if they end up being well-matched for your physiology, but a debacle if they aren’t.
The History & Science of HRT
The modern debate about HRT was shaped largely by the Women’s Health Initiative (WHI) trial published in 2002.
The study, performed on 16,608 women aged 50-79 years old, reported increased risks for:
- breast cancer
- stroke
- blood clots
Women with a uterus were given CEE + MPA daily, while women without a uterus were given CEE only. (CEE is animal derived estrogen, and MPA is synthetic progesterone.)
The reported increase in risks triggered a dramatic drop in hormone therapy use worldwide. However, later analysis revealed an important limitation. The average age of participants was 63, meaning many women started therapy more than a decade after menopause.[29]
This led researchers to propose the “timing hypothesis.”
The Timing Hypothesis
The timing hypothesis suggests that the person’s age and timeline into menopause may significantly affect risks and benefits of HRT. As summarized in a 2024 literature review on HRT[30]:
- “As women enter menopause, they begin to build up plaque and develop atherosclerosis… If therapy is started before these plaques begin to build, hormone therapy can have a positive effect on heart health. If it is started after these plaques have begun formation, therapy may have a negative effect.”
- “These results support the conclusion that timing of HRT should be initiated within six years of menopause to provide cardiovascular benefit.”
The formal WHI Timeline, with a Surprise 2026 Ending
This timeline has been carefully documented in recent clinician-oriented timelines[31]:
- 1993 – WHI study begins
- 2002, July – The trial is halted early. The combined estrogen + medroxyprogesterone acetate is causing more cancer and cardiovascular risk than potential benefits, in the older population.
- 2002, Summer & Fall – Widespread media coverage and influential publications contributed to a sharp reduction in HRT prescribing. (Even boxed warning label revisions were added in 2003.)
- 2003-2010’s – The “timing” or “window” hypothesis emerged: women closer to menopause initiation have different benefit–risk profiles than those initiating therapy later.[32,33]
- 2009-2020’s – New research is testing the new hypothesis
- Long-term WHI follow-up analyses and subsequent studies helped clarify how risks vary by formulation, dose, and timing.[34]
- Studies distinguished between systemic hormone therapies (oral or transdermal) and localized vaginal options, noting that lower-dose or regional delivery methods result in minimal systemic absorption.[35]
- Newer analyses of cardiovascular and dementia outcomes in younger women near menopause prompted recommendations to update treatment labeling.[36]
- 2025, November – FDA initiates reassessment of hormone-therapy boxed-warning language.
- The HHS/FDA[37] announced plans to review and revise boxed-warning language for some menopausal hormone therapy products, initiating a process to update labeling related to cardiovascular, breast cancer, and dementia risks.[38]
- ACOG statement: “ACOG commends the HHS leadership for improving the lives of perimenopausal women by making the estrogen products they need more accessible to them.”[39]
- The Menopause Society statement: “We agree with the FDA’s decision to remove the boxed warning on low-dose vaginal estrogen therapies used to treat genitourinary symptoms associated with menopause.”[40]
- WHI statement: “WHI does not have a position on the black box warning for menopausal hormone therapy. We note that in the years since the results of the WHI were published there has been no new information from similarly large randomized trials that would change the balance of known overall risks versus benefits for oral menopausal hormone therapy…The gold standard WHI trials showed that oral hormone therapy increased risks of stroke and blood clots and did not prevent heart attacks in women aged 50-79. In fact, during the first few years the risk of heart attacks was increased. In addition, combination estrogen plus progestin increased the risk of breast cancer irrespective of age and this risk became more significant over time in the trial and with longer duration of follow-up. Oral hormone therapy reduced diabetes and fracture risk, but increased risks of gallbladder disease, urinary incontinence and dementia in women over 65 years of age. For younger women, the benefit of vasomotor symptom reduction may outweigh the small cardiovascular risks, but it is uncertain whether any cardiovascular benefit seen in younger ages with estrogen alone will carry over into older ages as women and their arteries age. Our original conclusions still stand: oral menopausal hormone therapy should not be used for chronic disease prevention. Using menopausal hormone therapy for relief of moderate to severe vasomotor symptoms is reasonable but it should be limited to the lowest dose for the shortest time needed for this indication.”[41]
Just recently, and not (yet?) included in the above clinician timeline:
- 2026, February 6 (2026 JAMA) – The 9 living former members of the WHI data and safety monitoring board (DSMB) issue a warning: “Menopausal Hormone Labels Should Rely on Evidence, Not Opinion.”[42]
- Additional WHI Statement: “In a rebuke to the FDA, former WHI safety leaders warn that the agency’s quiet push to erase long‑standing hormone‑therapy warnings could put millions of women at risk. The authors call for a true, transparent advisory panel before this rushed overhaul that risks leaving women unaware of real, evidence‑based safety concerns.”[43]
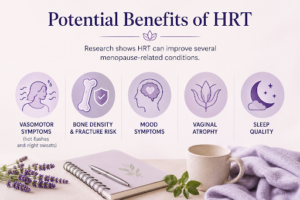
Potential Benefits of HRT
Research shows HRT can improve several menopause-related conditions[44]:
- vasomotor symptoms (hot flashes and night sweats)
- bone density and fracture risk
- mood symptoms
- vaginal atrophy
- sleep quality
“HRT also significantly decreases the incidence of various symptoms of menopause and the risk of osteoporotic fractures, and improves quality of life.”[45]
- Mikkelsen. BMJ.[46] OBSERVATIONAL STUDY
- This observational cohort study included 876,805 Danish women born between 1950 and 1977, followed from age 45 years, of whom 104,086 (11.9%) used menopausal hormone therapy and 47,594 (5.4%) died during follow-up. The “typical” participant in the study was observed for about 14 years.
- Conclusion: “This nationwide cohort study did not find menopausal hormone therapy was associated with increased mortality.”
- Dong. Obstetrics & Gynaecology.[47] REVIEW
- This narrative review suggests that, although HRT is prescribed primarily for menopausal symptom relief rather than for cardiovascular prevention, it may offer meaningful metabolic benefits during the menopausal transition, including attenuation of visceral fat accumulation, generally favorable effects on lipid profile, improved glycaemic control, and possible reduction in new-onset type 2 diabetes, with some evidence that route, timing, and progestogen choice influence the magnitude of benefit.
- Conclusion: “Whilst better non-hormonal treatments for menopausal symptoms are on the horizon, HRT remains the most effective treatment for menopausal symptoms and it is crucial for prescribers to be aware of the latest guidelines and areas of uncertainty in the evidence base.”
- The “better” treatments are referring to: Fezolinetant, a non-hormonal, prescription, neurokinin 3 (NK3) receptor antagonist used to treat hot flashes and night sweats.[48]
When initiated near menopause, cumulative evidence reviewed in the literature[49] suggests potential reductions in:
- coronary heart disease
- all-cause mortality
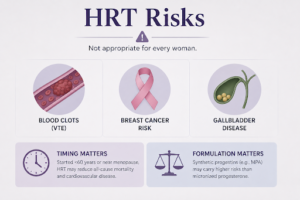
HRT Risks
Despite these benefits, HRT is not appropriate for every woman.
Potential risks include[50]:
- venous thromboembolism (blood clots)
- breast cancer risk
- gallbladder disease
“The totality of evidence indicates menopausal hormone replacement therapy (HRT) effects are determined by timing of initiation according to age and/or time since menopause, underlying health of target tissue, and duration of therapy. Initiated in women at younger than 60 years and/or at or near menopause, HRT significantly reduces all-cause mortality and cardiovascular disease (CVD), whereas other primary CVD prevention therapies such as lipid-lowering fail to do so.”
Formulation also matters. Synthetic progestins, such as medroxyprogesterone acetate used in the WHI study, appear to carry higher risk signals than micronized progesterone.[51]
Current Clinical Guidelines
Modern guidelines attempt to balance benefits and risks.
- The ACOG welcomed the policy change (removing the warning labels), saying it should improve access to estrogen therapy for perimenopausal women who need it.
- The Menopause Society supported removing the boxed warning for low-dose vaginal estrogen used to treat genitourinary symptoms of menopause.
- WHI said its original conclusions still stand: oral menopausal hormone therapy should not be used for chronic disease prevention, though short-term, low-dose use for significant menopausal symptoms can still be reasonable.

More specifically, the Menopause Society states a more exact timeframe for who should consider HRT:
- “For women aged younger than 60 years or who are within 10 years of menopause onset and have no contraindications, the benefit-risk ratio is favorable for treatment of bothersome vasomotor symptoms and prevention of bone loss.”[52]
- However, The Menopausal Society also warns that: “For women who initiate hormone therapy more than 10 years from menopause onset or who are aged older than 60 years, the benefit-risk ratio appears less favorable because of the greater absolute risks of coronary heart disease, stroke, venous thromboembolism, and dementia.”
Is HRT the better choice for you or your client
A Practical Framework for Women
Here is a helpful framework for making a decision about HRT.
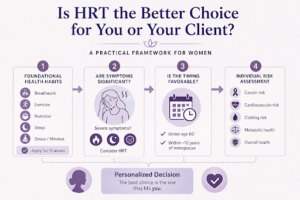
Step 1: Have foundational health habits already been applied?
- Breathwork
- Exercise
- Nutrition
- Sleep
- Stress / Mindset

Implementing or tweaking one of the above foundational habits may be enough to reduce menopausal symptoms. Especially if symptoms are mild to moderate, taking 12 weeks to implement the above baseline habits is a good idea not only for menopausal symptoms, but for quality of life – longevity – for the rest of one’s life.
Implementing or tweaking one of the above foundational habits may be enough to reduce menopausal symptoms. Especially if symptoms are mild to moderate, taking 12 weeks to implement the above baseline habits is a good idea not only for menopausal symptoms, but for quality of life – longevity – for the rest of one’s life.
Step 2: Are symptoms significant?
Hot flashes, sleep disruption, and quality-of-life impairment are the most common reasons to consider therapy. Especially if symptoms are severe, HRT is a valid option.
Step 3: Is the timing favorable?

Most guidelines[53] consider therapy more favorable for women:
- under age 60
- within about 10 years of menopause
When is it too late to start HRT, based on my age and menopausal status?
Clinicians may sometimes use the terms “early” and “late” stage menopause. The following definitions are an effort to help clarify:
- Perimenopause – Common ages 40 – 47; irregular periods.
- Early Menopause – Once 12 consecutive months of no period occurs, a person is considered menopausal, or postmenopausal. Up to about 10 years without menstruation is still considered “early initiation” for HRT. Common ages 47 – 51, and then to 61.
- Late Menopause – Late Postmenopause. Common age 61+. The adjusted WHI timing theory considers this to be too late for HRT.
Here is a specific example of the 10 years framework:
- Age 49 – irregular cycles (perimenopause)
Age 51 – last menstrual period
Age 52 – officially menopausal (12 months no period) - The “10-year window” runs roughly:
- Age 51 → Age 61
- Starting HRT anywhere in this window is what guidelines call the “early initiation” group.
Step 4: Individual risk assessment
Factors considered include:
- Cancer risk (especially hormone-sensitive cancers): personal history of breast cancer or endometrial cancer, BRCA (breast cancer) mutation carriers, family history of breast cancer.
- Estrogen plus progestin HRT has consistently shown an increase in breast cancer risk among postmenopausal women.[54]
- However, estrogen-alone HRT has little impact on breast cancer risk in naturally menopausal women, and in those who have had their uterus removed.[55]
- Cardiovascular risk: If you have established coronary artery disease (CAD), a prior stroke, peripheral vascular disease, are >10years menopause, or are age >60 years.
- Clotting risk: prior deep vein thrombosis (DVT) or pulmonary embolism (PE), known thrombophilia, antiphospholipid syndrome, strong clotting family history, or obesity + immobility + smoking.
- Overall metabolic health – insulin resistance, visceral adiposity, poor lipid status, non-alcoholic fatty liver disease, high inflammatory burden. Baseline metabolic health may influence both safety profile and treatment response to HRT.
- Overall health[56] – (nervous system stability, liver function, sleep quality, chronic disease burden). More resilient systems tend to tolerate systemic therapies with fewer adverse effects and more predictable outcomes.
What Happens When HRT Is Stopped?
What happens to the symptom relief benefits after stopping HRT?
Hormone therapy does not permanently reverse the underlying hormonal transition.
When therapy stops, many benefits may diminish.
“It has been shown that the benefits of estrogen decrease after discontinuing HRT.”[57] Symptoms such as hot flashes and bone loss may gradually return if no other interventions are implemented.
What happens to disease rates after stopping HRT?
Overall, after stopping hormone therapy, most risks and benefits appear to dissipate over time.[58,59]
- Breast Cancer: Risk risk appears to diminish after discontinuation of HRT.
- “The increased risk of breast cancer associated with the use of estrogen plus progestin declined markedly soon after discontinuation of combined hormone therapy.”[60]
- Cardiovascular risk appears to increase in the first year after stopping HRT, but reduces in risk after one year.
- “Within the first posttreatment year, the risk of cardiac death was significantly elevated…whereas follow-up for longer than 1 year was accompanied with a reduction…”[61]
- Fracture risk does not appear to return after stopping HRT.
- “We found no evidence for increased fracture risk, either sustained or transient, for former HT users compared with former placebo users after stopping HT. There was residual benefit for total fractures in former HT users from the CEE-alone study.”[62] (CEE – Conjugated equine estrogen)

Final Perspective
Menopause is a natural biological transition with consequences that affect multiple physiological systems. Hormone therapy is one potential tool.
Lifestyle factors such as exercise, nutrition, sleep, and stress regulation remain foundational.
For some women — particularly those with significant symptoms and low baseline risk — carefully selected hormone therapy may provide meaningful benefits when started near or prior to menopause.
Wanting to learn more holistic perspective on HRT, please view this followup article: “Menopause Symptom Solutions part 2: Timing, Formulations & Individualized HRT“
—————————–
If you love fun & research-based guidance as a fitness professional, or during your own pregnancy & postpartum, please check out these Fit For Birth offerings:
- For Fitness & Wellness Professionals:
- FREE 2-hour CEC
- CEC/CEU Courses, including our Pre & Postnatal Corrective Exercise Specialist (PPCES), the world’s first holistic perinatal CEC/CEU!
- Monthly Elite Membership – Community. Monthly education. Business mentorship & work opportunities. $27/month.
- For Pregnancy, Pre-conception & Postpartum:
- For Longevity:
—————————————————-
James Goodlatte is a Father, Holistic Health Coach, Corrective Exercise Practitioner, Speaker, Author, Educator, and the founder of Fit For Birth and Exercise For Longevity. Since 2008, when he found out he would be a father, his passion for holistic wellness shifted to children and families. Today, he is a driving force in providing Continuing Education Credits for the pre and postnatal world, with Fit For Birth professionals in 64 countries. James is a member of the First 1000 Days Initiative at the Global Wellness Institute, and professional longevity researcher & educator.
REFERENCES
[1] 2025. Wegrzynowicz, et al. Women (Basel). Retrieved 1/11/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC12014197/
[2] 2025. Wegrzynowicz, et al. Women (Basel). Retrieved 1/11/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC12014197/
[3] 2011. Prior, JC. Facts, Views, & Vision in ObGyn. “Evidence shows that with disturbed brain-ovary feedbacks, E2 levels average 26% higher and soar erratically – some women describe feeling pregnant! Also, ovulation and progesterone (P4) levels become insufficient or absent. The most symptomatic women have higher E2 and lower P4 levels.” Retrieved 1/14/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC3987489/
[4] 1998. Klein & Soules. Clinical Obstetrics and Gynecology. “The degree of unpredictability of the perimenopause is such that the diagnosis of menopause can only be made retrospectively.” Retrieved 1/14/26 from https://journals.lww.com/clinicalobgyn/abstract/1998/12000/endocrine_changes_of_the_perimenopause.17.aspx
[5] 2026, March 3. Fasting, Fat-loss, and Perimenopause. Fit For Birth Article. Retrieved 3/16/26 from https://getfitforbirth.com/fasting-fat-loss-and-perimenopause/
[6] 2009. Al-Azzawi. Palacios. Maturitas. Hormonal Changes During Menopause. “…attesting to the negligible role of postmenopausal ovaries in progesterone production…” Retrieved 3/16/26 from https://www.sciencedirect.com/science/article/abs/pii/S037851220900098X
[7] 1973. J. M. GRODIN, P. K. SIITERI, P. C. MACDONALD, Source of Estrogen Production in Postmenopausal Women, The Journal of Clinical Endocrinology & Metabolism, Volume 36, Issue 2, 1 February 1973, Pages 207–214, https://doi.org/10.1210/jcem-36-2-207
[8] 2013. Thomas. Rajiv Gandhi University of Health Sciences (India). Retrieved 3/16/26 from https://www.proquest.com/openview/0b7563e0333eebd53f0955a31c2e6ecf/1?pq-origsite=gscholar&cbl=2026366&diss=y
[9] 2018. Iyyappan et al. TNNMC Journal of Obstetrics and Gynaecological Nursing. Retrieved 3/16/26 from https://indianjournals.com/article/tnnmcjogn-6-2-002
[10] 2014. Sternfeld, et al. The Journal of The Menopause Society. Retrieved 3/16/26 from https://journals.lww.com/menopausejournal/abstract/2014/04000/efficacy_of_exercise_for_menopausal_symptoms__a.5.aspx
[11] 2020. Nguyen et al. Exercise and Quality of Life in Women with Menopausal Symptoms: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. IJERPH. Retrieved 3/16/26 from https://www.mdpi.com/1660-4601/17/19/7049
[12] 2022. Berin, E., Spetz Holm, AC., Hammar, M. et al. Postmenopausal women’s experiences of a resistance training intervention against vasomotor symptoms: a qualitative study. BMC Women’s Health 22, 320. https://doi.org/10.1186/s12905-022-01900-0
[13] 2022. Berin, E., Hammar, M., Lindblom, H., Lindh-Åstrand, L., & Spetz Holm, A. C. Effects of resistance training on quality of life in postmenopausal women with vasomotor symptoms. Climacteric, 25(3), 264–270. https://doi.org/10.1080/13697137.2021.1941849 Retrieved 3/16/26 from https://www.tandfonline.com/doi/full/10.1080/13697137.2021.1941849#abstract
[14] 2023. Capel-Alcaraz, et al. Journal of Clinical Medicine. Retrieved 3/16/26 from https://www.mdpi.com/2077-0383/12/2/548
[15] 2024. Erdélyi, et al. Nutrition and Hormone Regulation. Nutrients 2024, 16(1), 27; https://doi.org/10.3390/nu16010027 Retreived 3/17/26 from https://www.mdpi.com/2072-6643/16/1/27
[16] 2025. Yang, et al. Nutrients 2025, 17(2), 356; https://doi.org/10.3390/nu17020356 Retrieved 3/17/26 from https://www.mdpi.com/2072-6643/17/2/356
[17] 2015. Tal et al. Current Psychiatry Reviews. Retrieved 3/17/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC4607064/
[18] 2020. Xu, Q., Esterman, A., Dorrian, J., & Warland, J. (2020). An examination of the relationship between sunlight exposure and hot flush in working women. Chronobiology International, 37(3), 425–437. https://doi.org/10.1080/07420528.2020.1737101
[19] 2025. Menezes-Júnior et al. BMC Public Health. Retrieved 3/17/26 from https://link.springer.com/article/10.1186/s12889-025-24618-8
[20] 2017. Stefanopoulou. Grunfeld. Journal of Psychosomatic Obstetrics & Gynecology. Retrieved 3/16/26 from https://www.tandfonline.com/doi/abs/10.1080/0167482X.2016.1235147
[21] 2020. Thomas et al. Journal of Clinical & Diagnostic Research. REVIEW. Retrieved 3/16/26 from https://openurl.ebsco.com/EPDB%3Agcd%3A13%3A32053245/detailv2?sid=ebsco%3Aplink%3Ascholar&id=ebsco%3Agcd%3A144764171&crl=c&link_origin=scholar.google.com // DOI: 10.7860/JCDR/2020/43721.13831
[22] 2021. Langer, R. D., Hodis, H. N., Lobo, R. A., & Allison, M. A. Hormone replacement therapy – where are we now? Climacteric, 24(1), 3–10. https://doi.org/10.1080/13697137.2020.1851183
[23] 2012. Goodman, et al. Journal of Women’s Health. Sage Journals. Retrieved 3/17/26 from https://journals.sagepub.com/doi/full/10.1089/jwh.2011.2839
[24] 1993. W L Kraus, B S Katzenellenbogen, Regulation of progesterone receptor gene expression and growth in the rat uterus: modulation of estrogen actions by progesterone and sex steroid hormone antagonists, Endocrinology, Volume 132, Issue 6, 1 June 1993, Pages 2371–2379, https://doi.org/10.1210/endo.132.6.8504742
[25] 2007. Fugh-Berman, A., Bythrow, J. Bioidentical Hormones for Menopausal Hormone Therapy: Variation on a Theme. J GEN INTERN MED 22, 1030–1034 (2007). https://doi.org/10.1007/s11606-007-0141-4
[26] 2018. Allan E Herbison, The Gonadotropin-Releasing Hormone Pulse Generator, Endocrinology, Volume 159, Issue 11, November 2018, Pages 3723–3736, https://doi.org/10.1210/en.2018-00653
[27] 1993. J.C. Marshall, M.L. Griffin, The role of changing pulse frequency in the regulation of ovulation, Human Reproduction, Volume 8, Issue suppl_2, 1 November 1993, Pages 57–61, https://doi.org/10.1093/humrep/8.suppl_2.57
[28] 2013. L’Hermite. Climacteric. HRT optimization, using transdermal estradiol plus micronized progesterone, a safer HRT. Retrieved 3/17/26 from https://www.tandfonline.com/doi/abs/10.3109/13697137.2013.808563
[29] 2012. Position Statement. Menopause: The Journal of The North American Menopause Society 19(3):p 257-271, March 2012. | DOI: 10.1097/gme.0b013e31824b970a // https://pubmed.ncbi.nlm.nih.gov/22367731/
[30] 2024. Kleinschmit, Hannah. South Dakota University. An Overview of Women’s Hormone Replacement Therapy (HRT). Retrieved 3/17/26 from https://openprairie.sdstate.edu/honors_isp/20/
[31] 2025. Halsey, Grace. Hormone Replacement Therapy After the WHI: Clinician’s Evidence Timeline (2002–2025) Patient Care. Retrieved 3/16/26 from https://www.patientcareonline.com/view/hormone-replacement-therapy-after-the-whi-clinician-s-evidence-timeline-2002-2025-
[32] 2013. Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368. doi: 10.1001/jama.2013.278040 // https://jamanetwork.com/journals/jama/fullarticle/1745676
[33] 2013. Clarkson TB, Meléndez G, Appt SE. Timing hypothesis for postmenopausal hormone therapy: its origin, current status, and future. Menopause. 2013;20(3):342‑353. doi: 10.1097/gme.0b013e3182843aad // https://pubmed.ncbi.nlm.nih.gov/23435033/
[34] Shufelt CL, Bairey Merz CN, Ross L, et al. Hormone therapy dose, formulation, route of delivery, and risk of cardiovascular events in women: findings from the Women’s Health Initiative Observational Study. Menopause. 2014;21(3):260‑266. https://pubmed.ncbi.nlm.nih.gov/24045672/
[35] 2022. Goldštajn MS, Mikuš M, Ferrari FA, et al. Effects of transdermal versus oral hormone replacement therapy in postmenopause: a systematic review. Arch Gynecol Obstet. 2022 Jun 17;307(6):1727–1745. doi: 10.1007/s00404-022-06647-5 // https://pubmed.ncbi.nlm.nih.gov/35713694/
[36] 2019. Oliver‑Williams C, Glisic M, Shahzad S, et al. The route of administration, timing, duration and dose of postmenopausal hormone therapy and cardiovascular outcomes in women: a systematic review. Hum Reprod Update. 2019;25(2):257‑271. doi: 10.1093/humupd/dmy039 // https://pubmed.ncbi.nlm.nih.gov/30508190/
[37] FDA = Food & Drug Administration. The FDA is part of the HHS, Health & Human Services.
[38] 2026, Feb. 12. FDA News Release. “FDA Approves Labeling Changes to Menopausal Hormone Therapy Products.” Retrieved 3/16/26 from https://www.fda.gov/news-events/press-announcements/fda-approves-labeling-changes-menopausal-hormone-therapy-products
[39] 2025, Nov. 10. ACOG News Release. Retrieved 3/16/26 from https://www.acog.org/news/news-releases/2025/11/acog-president-says-label-change-on-estrogen-will-increase-access-to-hormone-therapy
[40] 2025, Nov. 10. The Menopause Society Press Room. Retrieved 3/16/26 from https://menopause.org/press-releases/the-menopause-society-comments-on-the-fda-announcement-on-hormone-therapy
[41] November 10, 2025. News from the WHI Study. November 2025 | FDA announced changes to the FDA labeling for Menopausal Hormone Therapy. Retrieved 3/16/26 from https://www.whi.org/md/news/whi-fda-hrt-warning
[42] 2026. Wittes J, Braunwald E, Chesney MA, et al. Menopausal Hormone Labels Should Rely on Evidence, Not Opinion. JAMA. Published online February 06, 2026. doi:10.1001/jama.2026.1308 // https://jamanetwork.com/journals/jama/article-abstract/2844960
[43] February 2026 | Former WHI DSMB Members publish a Viewpoint in JAMA: Menopausal Hormone Labels Should Rely on Evidence, Not Opinion. News from the WHI Study. November 2025 | FDA announced changes to the FDA labeling for Menopausal Hormone Therapy. Retrieved 3/16/26 from https://www.whi.org/md/news/whi-fda-hrt-warning
[44] Lobo, R. Hormone-replacement therapy: current thinking. Nat Rev Endocrinol 13, 220–231 (2017). https://doi.org/10.1038/nrendo.2016.164
[45] Lobo, R. Hormone-replacement therapy: current thinking. Nat Rev Endocrinol 13, 220–231 (2017). https://doi.org/10.1038/nrendo.2016.164
[46] 2026. Mikkelsen. BMJ 2026;392:e085998 Retrieved 3/17/26 from https://www.bmj.com/content/392/bmj-2025-085998.abstract
[47] 2026. Dong et al. Obstetrics & Gynaecology. Retrieved 3/17/26 from https://obgyn.onlinelibrary.wiley.com/doi/full/10.1111/1471-0528.70214
[48] 2023. Lee, A. Fezolinetant: First Approval. Drugs 83, 1137–1141 (2023). https://doi.org/10.1007/s40265-023-01917-1
[49] 2022. Hodis. Mack. The Cancer Journal 28(3):p 208-223, 5/6 2022. | DOI: 10.1097/PPO.0000000000000591 Retrieved 3/17/26 from https://journals.lww.com/journalppo/abstract/2022/05000/menopausal_hormone_replacement_therapy_and.9.aspx?context=latestarticles
[50] 2021. Zhang, et al. PLOS Medicine. Menopausal hormone therapy and women’s health: An umbrella review. Retrieved 3/17/26 from https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003731
[51] 2021. Hipolito Rodrigues, M. A., & Gompel, A. (2021). Micronized progesterone, progestins, and menopause hormone therapy. Women & Health, 61(1), 3–14. https://doi.org/10.1080/03630242.2020.1824956
[52] “The 2022 Hormone Therapy Position Statement of The North American Menopause Society” Advisory Panel. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022 Jul 1;29(7):767-794. doi: 10.1097/GME.0000000000002028 // PMID: 35797481. // https://pubmed.ncbi.nlm.nih.gov/35797481/
[53] 2020. J Menopausal Med. 2020 Aug 31;26(2):69–98. doi: 10.6118/jmm.20000 Retrieved 3/17/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC7475284/
[54] 2025. Kim & Munster. Annals of Oncology. Retrieved 5/10/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC12168202/ doi: 10.1016/j.annonc.2024.10.824
[55] 2025. Kim & Munster. Annals of Oncology. Retrieved 5/10/26 from https://pmc.ncbi.nlm.nih.gov/articles/PMC12168202/ doi: 10.1016/j.annonc.2024.10.824
[56] 2020. Costa et al. Influence of Menopausal Hormone Therapy on Body Composition and Metabolic Parameters. Retrieved 3/17/26 from https://journals.sagepub.com/doi/full/10.1089/biores.2019.0050
[57] 2024. Kissinger, Dohn. Hormone Replacement Therapy Perspectives. Frontiers in Global Women’s Health. https://doi.org/10.3389/fgwh.2024.1397123
[58] 2011. Taylor. Manson. The Journal of Clinical Endocrinology & Metabolism, Volume 96, Issue 2, 1 February 2011, Pages 255–264, https://doi.org/10.1210/jc.2010-0536
[59] Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal Hormone Therapy and Health Outcomes During the Intervention and Extended Poststopping Phases of the Women’s Health Initiative Randomized Trials. JAMA. 2013;310(13):1353–1368. doi:10.1001/jama.2013.278040 Retrieved 3/17/26 from https://pubmed.ncbi.nlm.nih.gov/24084921/
[60] 2009. Chlebowski, et al. N Engl J Med. Breast Cancer after Use of Estrogen plus Progestin in Postmenopausal Women. 2009;360:573-587 DOI: 10.1056/NEJMoa080768 Rtrieved 3/17/26 from https://pubmed.ncbi.nlm.nih.gov/19196674/
[61] 2015. Mikkola et al. The Journal of Clinical Endocrinology & Metabolism, Volume 100, Issue 12, 1 December 2015, Pages 4588–4594, https://doi.org/10.1210/jc.2015-1864
[62] 2017. Nelson B. Watts, Jane A. Cauley, Rebecca D. Jackson, Andrea Z. LaCroix, Cora E. Lewis, JoAnn E. Manson, Joan M. Neuner, Lawrence S. Phillips, Marcia L. Stefanick, Jean Wactawski-Wende, Carolyn Crandall, for the Women’s Health Initiative Investigators, No Increase in Fractures After Stopping Hormone Therapy: Results From the Women’s Health Initiative, The Journal of Clinical Endocrinology & Metabolism, Volume 102, Issue 1, 1 January 2017, Pages 302–308, https://doi.org/10.1210/jc.2016-3270