Last Updated 3/4/25
Common Triggers of SI Joint Pain and How to Prevent a Flare-up | Spine-health
Sacroiliac joint (SIJ) pain arises from the SI joint, where the spine meets the pelvis. It can be debilitating and impact daily activities. Understanding the common triggers and preventive measures can help manage and reduce the frequency of flare-ups.
Here are the two things that you come away understanding from this article:
- The underlying cause of SIJ pain & dysfunction is misalignment of the joint, correlated to poor muscle function in the SIJ area.
- The most appropriate first-response to SIJ pain & disability is corrective exercise. Your exercises are made far more effective when you know exactly which muscles are overactive, which are underactive, and also which side SIJ is either too locked/immovable or too loose/unstable.
This article will teach you a bit about SIJ, pelvic & spine health, before ultimately teaching you how to select some exercises that are right for you. If at any point along the way, you want a professional assessment to help create your individualized SIJ healing program, please consider our 2-session online assessment & corrective exercise starter package.

Common Triggers of SI Joint Pain
The SI joint can become misaligned for various reasons. Here are some of them:
- Trauma: A fall, accident, or sudden impact that jolts the lower back can move the SI joint out of place. Labor & delivery of childbirth is also a potential trigger “event” that moves the SIJ out of alignment.
- Improper Biomechanics: Poor posture or muscle imbalances can put extra stress on the SIJ, causing the joint to either be stuck in place, or hypermobile. Carrying a fetus changes the muscle length-tension relationships as well, which alters the positioning of the SIJ.
- Physical Strain & Overuse: Activities that involve prolonged standing, or excessive repetitive movements can lock the SIJ, or produce excessive movement in the SIJ and surrounding muscles, leading to pain.
- Pregnancy: The body releases hormones during pregnancy that allow ligaments to relax and stretch in preparation for childbirth. This can cause increased movement (hyper mobility) in the joints and can lead to instability and pain in the SIJ specifically.
- Arthritis: Degenerative arthritis or osteoarthritis can develop in the SIJ, causing wear and tear that leads to pain and stiffness. Note that this degeneration is often itself caused by the joint not being aligned properly.
- Inflammatory Joint Disease: Conditions like ankylosing spondylitis or psoriatic arthritis can cause inflammation in the SI joints, leading to chronic pain.
How to Prevent a Flare-Up
The root cause of preventing SIJ pain and disability is to activate the underactive muscles in the pelvic area, while relaxing the overactive muscles. Doing so will allow locked SI joints to restore proper movement, and allow unstable SI joints to restore proper stability. This is the foundation of corrective exercise. Here is an overview of ideas to consider in your life:
- Align your SIJ: Determine if your SIJ is locked into too little movement, or hypermobilized into excessive movement. Using this information, you can perform specific exercises to either stabilize the hypermobility, or mobilize the locked area.
- Daily Stability Training: Perform exercises that specifically align your body. While some exercises are critical for nearly all cases of SI Joint Pain (like strengthening glutes and core), some will be very individualized for you (like needing to stretch the left hip external rotators, right internal rotators, and maybe one inner thighs more than the other). Start with the ones you know, and consider getting an individualized assessment.
- Strengthen Proper Posture: Posture is being formed and re-formed moment by moment. Be mindful to maintain a posture that supports the natural vertical S-curve of your spine, while sitting, standing, and living life.
- Exercise Regularly: Being sedentary degrades postural muscles, so we need to “use them or lose them.” Avoid the slide into sedentary weakness by picking an activity that you enjoy, and aim to do it regularly.
- Avoid Strain in normal life activities: Make sure you know how to activate your glutes when lifting, or your obliques when running or pulling, etc. Using the correct muscles in daily activities means that less strain will appear in the joints. In many cases, your very first activation can reduce pain dramatically.
- Pain is Communication: If certain activities or exercises cause pain, modify them to avoid aggravating the SI joint. Seek alternative exercises that do not stress this area.
- Supportive Devices: Devices like braces and belts are helpful in stabilizing your SI Joint in the acute stages of pain. Just remember that true strength means learning to use the correct muscles, rather than relying on an external support. (This same concept applies to leg length discrepancies, which are usually developed over time due to muscle imbalances. It is commonly observed in clinical settings that these are far more common than an actual anatomical difference in the length of the leg bones.)
- Manual Therapy: A manual therapist can physically manipulate your body, releasing tight fascia, or literally adjusting the bones around your SI Joint.
Implementing these strategies can help manage and potentially reduce the frequency of SI joint pain flare-ups, improving overall quality of life.
Proper Spine & Pelvic Health
The overall well-being and functional integrity of your spine & pelvis is crucial for you to live without chronic pain, all the days until you die peacefully in your sleep one day.
There are two basic skills that your spine & pelvis must be able to accomplish in all three dimensions of movement, consistently, and on-time:
- Stability – Ability to lock the position of the spine & pelvis in place – without compression, tension or shearing – while performing any movement.
- Mobility – Flexibility with enough strength to hold strong at end ranges of motion.
At any given time, hundreds of muscles are working together to create the appropriate positioning for your joints, including those around the spine & pelvis. If performing a heavy deadlift in the gym, for example, it’s most common that your corrective exercise specialist would want your inner unit & outer unit core muscles to synchronize in their muscle activation, specifically to keep the natural S-curve of the spine from moving at all. (This is called spinal stability.) In the case of a “straight-leg deadlift”, we are looking for basically all joints to be perfectly stable (non-moving), except for the ball-in-socket hip joint, which hinges to allow the deadlift exercise to happen.

Photo by Anastase Maragos on Unsplash
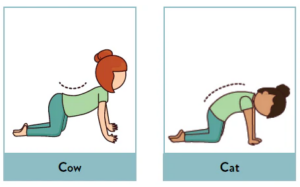
When trying to produce “stability”, one’s musculature should not allow the bones of the spine or pelvis to be permitted to move. On the flip side, there are spinal segmentation exercises that intend to require the spine to move vertebrate by vertebrate, rather literally. Think of being on hands & knees and doing the common cat-cow exercises, but really focused on segmentally moving one vertebrae at a time. This kind of exercise “mobilizes” the spine, by intending to gain more movement, typically between every spinal segment. Since mobility is the combination of having the flexibility to create a full range of motion, while simultaneously having the strength to hold and control it, exercises like cat-cow can be useful for spinal health.
In other words, learning to brace the pelvis & spine in a non-moving position locks the segments in place, preventing them from grinding on each other. Mobility can also be part of the corrective process, but only if you identify – through an individualized assessment – which exact areas of your spine & pelvis actually need to be mobilized. (ie. identifying which areas are stuck, and “un-stucking” them, will absolutely reduce the typical over-mobility happening in other joint areas.)
This is why renowned back pain experts, like Dr. Stuart McGill, renowned professor of spine biomechanics, teaches that the “core…muscles act to stiffen the torso and function primarily to prevent motion.”[2] Especially when pain is present, we generally will first teach our clients to stabilize.
But in the case of SIJ pain and disability, the kinds of exercises you choose depends whether or not the SIJ is locked into too little movement, or unstable because of too much movement.
What Is the SI Joint?
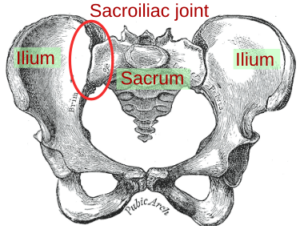
A joint is where two bones meet. In the case of the sacroiliac joint (SI joint / SIJ), the two bones meeting are the sacrum and the ilium. The sacrum bone sits at the base of your spine, and is made of 5 fused vertebrae, while the ilium is part of the pelvic bone. Each person has two sacroiliac joints, one on each side of the sacrum, and their appropriate function is to have only limited, slight gliding movements (much less movement than the ball & socket of the shoulder, for example, but a bit more than the fixed joints of the skull).
The SIJ is heavily supported by strong ligaments that restrict its movement to provide stability to the pelvis. Despite being a fairly rigid joint, it allows for a small amount of movement, which is essential for effectively absorbing shock during walking and other activities, while also maintaining stability of the pelvis and spine.
SIJ Function includes:
- Transfer the load from upper to lower body.
- Shock absorbs the load, as it transfers.
- Mobility: Although the SI joints are not very mobile, their slight movements are important for accommodating movements such as bending and twisting. During childbirth, the flexibility of these joints increases due to hormonal changes, allowing for easier passage of the baby.
| Too much or too little, or just right?
The SI joints can be a source of pain and discomfort when they move too much or too little. Although there are some cases where you may be able to discern which issue is at hand inside your own body, in most cases, an individualized assessment is necessary to help you figure this out. When the SIJ becomes inflamed – from movement that is either too limited or too hypermobile – conditions such as SI joint dysfunction (abnormal movement of the joint) or sacroiliitis (inflammation of the SI joints), and pain, occurs. |
Relation of si joint dysfunction and pregnancy
Since pregnancy changes the muscle balance of the body, specifically affecting the pelvis, SI joint pain is highly correlated. While there are pregnancy-related pelvic changes that affect “everyone” there can also be changes that are unique to the individual. This is why some pregnancies will have severe suffering of SI joint pain, while others experience no discomfort at all, or even a reduction in previous symptoms.
During pregnancy, the body produces hormones such as relaxin, which helps to relax the ligaments in the pelvis and softens the cervix in preparation for childbirth. These changes can lead to increased mobility and instability in the SI joints. This increased laxity can cause misalignment and abnormal movement at the SIJ, leading to pain and discomfort.
Also, as the uterus expands, it adds weight and shifts the center of gravity forward, increasing the curve of the lower back (lumbar lordosis). For women who are already excessively tilted lordotically, this extra shift places additional stress on the SI joints and can exacerbate instability and pain in these areas. Interestingly, women whose pelvis alignment is already tucked under may experience a balancing effect, as the lordosis actually can pull them into better alignment.
What SI Joint Pain Feels Like
Sacroiliac (SI) joint pain can vary, but there are common symptoms that people typically experience. Here’s what SI joint pain often feels like:
- Location of Pain: SI joint pain usually occurs in the lower back and buttocks. It can affect one side or both sides of the body, though it often affects just one side more prominently. It often starts in the SI joint area and may radiate into the buttocks, hips, groin, or even down the back of the thigh. However, it usually doesn’t extend past the knee.
- Nature of Pain: The pain can be sharp, stabbing, or dull in nature.
- Aggravating Factors: The pain is typically worsened by prolonged standing, stair climbing, lying down, or any activities that involve putting weight on one leg more than the other. Transition movements, such as standing up from a sitting position or turning in bed, can also provoke discomfort.
- Stiffness and Reduced Range of Motion: People may experience stiffness or a burning sensation in the pelvis and lower back, which can reduce mobility and make daily activities challenging.
- Feeling of Instability: Some individuals report a sensation of instability in their pelvis, feeling as if their legs might buckle or that their pelvis is not supporting their upper body adequately.
- Alleviating Factors: Rest or changing positions often alleviates the pain. Applying heat or cold to the area can also provide temporary relief.
SI joint pain can sometimes be mistaken for other types of lower back pain, such as pain originating from the lumbar spine or hip issues. Therefore, accurate diagnosis is crucial for effective treatment.
Location of Pain may be an Identifier of how to Treat SIJ
To help you try to self-identify and treat your SIJ pain, it is helpful to know that a loose/unstable SIJ may tend to correlate to hip & groin pain, while a locked SIJ may tend to present as lumbar & sciatic-like pains.
- Hip & Groin Pain when SIJ is Hypermobile: When there’s too much movement at the SIJ, the joint instability can lead to feelings of pain in the lower back and hip, potentially radiating towards the groin. This type of pain is often due to the joint’s excessive movement stressing the surrounding ligaments and muscles.
- Lumbar & Radiating Pain when SIJ is Hypomobile: When there’s too little movement in the SIJ, the pain can be more localized to one side of the low back or buttocks and may radiate down the leg, similar to sciatica. This pain generally stays above the knee, but in some cases, it might extend to the ankle or foot. This occurs because the restricted movement at the SIJ can lead to muscle imbalances and increased stress on adjacent structures, which exacerbates pain distribution along the affected nerve pathways.
It’s handy to begin one’s hypothesis with the above information, but keep in mind that it is not always exact. Considering the function of the SI joint, the possibility of SIJ dysfunction prior to the onset of SIJ pain, and its potential pain referral patterns, “evaluation (and treatment) of the SI joint should be done regardless of where pain originates in lumbo-pelvic complex!”[4]
Misalignment Causes SI Joint Pain
“Sacroiliac (SI) joint dysfunction is a condition that happens when one or both small, firm joints at the base of the spine don’t move properly.”[5]
SIJ joint pain occurs when the joint is not in proper function and alignment. As noted above, this misalignment & improper function can be caused by trauma, improper mechanics/posture, physical strain, pregnancy and more. But underneath it all, you will find malfunction and misalignment.
Managing SIJ pain means you must address the underlying cause, so becoming aware of hyper- vs hypo-mobility in the SIJ is the main underlying strategy, followed by using corrective exercises until you are functioning at your best again.
What Exercises Should You Avoid for SI Joint Pain?
Compared to other treatments, exercises aimed at improving lumbopelvic stability are considered to have the most potential for reducing pain and disability from SIJ.[6] Steroid injections, radiofrequency ablation, stem cells, and even surgery are medical options,[7] but these should be reserved for those who are unable to find their solution with corrective exercise. This section will help you find your solution using stability exercises!
First, stop doing any exercises and movements that hurt. Although this will differ somewhat between individuals, there are a list of exercises that are more likely to exacerbate things. Here are some types of exercises you should generally avoid or modify if you’re experiencing SI joint pain:
- Any movement or exercise that already hurts, or that you suspect is reinforcing your specific joint hyper or hypomobility.
- Uneven Exercises (at first): Any exercise that works one side of the body more than the other, or uneven loading of weights, like a 1-legged squat, can contribute to or exacerbate SI joint imbalance and pain. A 2-legged squat will not put as much strain onto the SIJ that is out-of-alignment. Performing 1-legged squats, while necessary for human function under normal conditions, may be too much while you’re healing from your SIJ imbalance. To be clear, you must be able to get back to uneven exercises ASAP, it’s just that you may not be ready for those at first.
- Strength-training that pushes you beyond your ability to feel the correct muscles. (ie. you should feel glutes, not your low back muscles, and not pain.)
- High-Impact Activities/Plyometrics: Exercises that involve a lot of jumping or impact, such as running, jogging, box jumps, burpees, or high-impact aerobics, can be too jarring for sensitive SI joints.
- Hip Twisting Motions: Activities that involve twisting at the waist while standing, such as golf or some types of dance, can place additional stress on the SIJ.
- Some Yoga Poses: While yoga can be beneficial for flexibility and strength, certain poses that involve stretching or twisting the legs widely apart, such as Warrior poses or deep twists, might strain the SIJ.
| 2019 Study in Pain Physician Journal
Study Conclusion: “Exercise and manipulation therapy appear to be effective in reducing pain and disability in patients with SIJD. However, the combination of these 2 therapies does not seem to bring about significantly better therapeutic results than either approach implemented separately.”[8] Take home message: Corrective Exercises have a chance to be the only thing that you need in reducing your SIJ pain & disability! |
SI Joint Exercises to Prevent Injury
SI joint dysfunction is an imbalance in this musculo-skeletal area. As such, the best advice for healing, and preventing further exacerbation is to get a specific assessment, personalized for you. This will be able to tell you exactly which muscles you need to strengthen, and which stretches are critical for you.
While you are awaiting this appointment, and depending the severity of your symptoms, you can start in some of the most important areas:
- Strengthen your glutes.
- Strengthen your core.
- Apply your core breathing to all of your daily movements.
- You also may feel good about participating in low-impact cardio like cycling. Although this will not likely align your imbalance, it may be a useful form of getting a sweat through this challenging time.
Here are some specific exercises you can use for SIJ
Core Breathing Belly Pump
How to Do It: Lie on your back with your knees however comfortable. Inhale into your torso (lateral ribs, tummy, and lower back), and then exhale to create a smaller tummy. Extend your exhale for perhaps 3-5 seconds so that you feel your core muscles engage gently. If you’re pregnant, this exhale can be thought of as “hugging your baby.” Repeat 5-10 times, intending to make this a mild inner unit core exercise.
Supine Pelvic Tucks

How to Do it: Lay on your back with your knees bent. In conjunction with your core breathing, inhale to gently arch your back (creating a natural lordosis), and then exhale to tuck your pelvis (flattening your lumbar back, removing the lordosis). Most people should accentuate the tucking of the pelvis. If this position with the knees bent feels easy, you can straighten your knees until the challenge increases to an appropriate level. As you master the tuck with straight legs, you can progress to doing them while standing on 2-legs, and then eventually on 1-leg.
SI Joint-Friendly Tip: Make sure that you synchronize your movement to your core breathing. Most people erroneously move prior to any core activation, rather than properly activating core just prior to their movement. Don’t let this be you. Train your exhale to move your pelvic tuck in this exercise.
Side plank

How to Do It: Lay on your side with your legs extended. Prop your upper body up on your elbow, which will be directly under your shoulder. Stack your legs and feet together. Lift your hips off the ground, forming a straight line from your ankles to your shoulders. Hold this position for 30, 45, or 60 seconds each side. You can reduce the difficulty by bending your knees and lifting from a knee-supported position.
SI Joint-Friendly Tip: Feel free to rotate your body forward or backwards slightly, in order to place the tension more so into your obliques/abdominal muscles. In addition, consider which part of your leg muscles are holding you. Glutes, or lateral thighs? Choose the position without pain, but also see what you can do to nudge toward feeling more and more glutes over time.
Horse Stance or Bird dog

How to Do It: Start on all fours with your hands under your shoulders and knees under your hips. First, start by using your core breathing to lift one knee barely from the ground, just enough to slide a sheet of paper under that knee. Alternate legs several times, feeling for the stability/mobility in your SIJ. Try to feel your obliques stabilizing your core.
Second, use your core breathing to lift one hand barely from the ground, just enough to slide a sheet of paper under that hand. Alternate hands several times, feeling for the stability/mobility in your SIJ. Try to feel your obliques stabilizing your core.
Third, use your core breathing to lift one hand and the opposite knee simultaneously, barely from the ground, just enough to slide a sheet of paper under. Alternate this cross-connection several times, feeling for the stability/mobility in your SIJ. Try to feel your obliques stabilizing your core.
Finally, once you are regularly feeling your obliques stabilize for you, you can move onto a larger range of motion with your limbs. Slowly extend your right arm forward while simultaneously extending your left leg back. Lift both limbs level with your body, then return to the starting position and switch sides.
SI Joint-Friendly Tip: Most people will move their limbs “easily”, and never take the time for their core to learn how to stabilize. This is not intended to be a “hard” exercise. It is intended to train your natural inner core breathing system to activate prior to your movements. Most people are erroneously periphery-dominant, rather than properly core dominant. Do not let this be you.
Sidelying Clamshell
How to Do It: Lie on your side with your hips and knees bent at 45-degree angles, legs stacked. Keeping your feet together, raise the top knee as high as you can without shifting your hips or pelvis, then slowly lower it back down. The purpose of this exercise is for you to feel the deep hip rotator muscles (feels similar to your glutes).
SI Joint-Friendly Tip: Keep your pelvis stable and avoid rocking back as you lift and lower your knee. This stability is crucial to prevent aggravating the SI joint. You can place a hand on your hip to ensure it stays in place during the exercise. Also, connect your core breathing to this movement.
Supine Alternating Clamshell

How to Do It: Lay on your back with your knees bent. Keeping your feet on the floor, let your left knee open out toward the floor to the left, then bring it back to center. Then bring the right knee out toward the floor to the right, then back to center. Find a rhythmic soothing pace to gently pump fluid into the SI joint. This exercise is encouraging the muscles in this area to learn how to move without pain, and will possibly help to reposition the sacrum into a more ideal alignment.
Sidelying Hip Glides

How to Do It: Lay on your side, with your head comfortably supported, and your hips & knees bent to 90 degrees. When laying on your right side, gently rhythmically move your left hip & knee back a few inches, and then forward into starting position. Repeat in a soothing manner. Do on the other side as well. This exercise is encouraging the muscles in this area to learn how to move without pain, and will possibly help to reposition the sacrum into a more ideal alignment.
Seated Sit-Bone “Walking”
How to Do It: Sit cross-legged on your mat, but with bottoms of feet facing each other (rather than actually crossing your legs). “Waddle-walk” yourself forward, as if your sit-bones were your feet. You can “walk” forward and then backwards as well. This is an exercise that teaches the muscles around the SI joint to activate in more focused coordination.

Supine Lateral Ball Roll

How to Do It: Lay on a Swiss Ball in a classic glute bridge position, with your head & shoulders on the ball, and your glutes holding you up. Place your arms out to the side and bring shoulder blades together. Step your feet to the left just a bit, feeling the left glute engage, and allow your upper body to slide left along with the lower body. Hold for 10 seconds, return to the center, and then do the same thing to the right side. Repeat just a few times each side, intending to allow your glutes and your core breathing to connect.
| 2024 Systematic Review of Manual Therapy in SIJ Research Studies
What this Systematic Review is about: Manual therapy is a type of physical therapy that involves a skilled practitioner using their hands to manipulate soft tissues like muscles and joints, aiming to reduce pain, improve range of motion, and restore function in the musculoskeletal system. Essentially, manual therapy is a “hands-on” treatment, whereas corrective exercise is a do-it-yourself treatment. Results: According to a large analysis of 11 research studies: Manual therapy does improve disability, although not necessarily pain. More importantly, “compared to non-manual physiotherapy [like exercise]… SIJ manual therapy did not significantly reduce pain…”[9] Take Home Message: Especially with the right assessment, your at-home corrective exercises are as likely to be as effective as manual therapy! You may not need to go to a manual hands-on therapist. |
SI Joint Stretches to Ease Discomfort
A generalized set of stretching exercises is often counterproductive, as it could further destabilize already overly flexible areas as well as maintain discrepancies between the two sides of the body.[10]
When treating your own SIJ, you really need to assess yourself along the way, watching to see if your flexibility in any particular location is (a) obviously different than the other side of your body, and (b) short, compared to “normal” ranges.
To be clear, doing this on your own, you will often be able to determine where you are shorter on one side than another. However, where it gets more challenging, is if you’re not sure what normal ranges of motion should be at any given joint area. (This is where an individualized assessment will be most useful.)
| 2011 Case Study on Female SIJ patient[11]
Details of study: A 65-year old woman with a 10-month history of constant left lower back and leg SIJ pain. This patient was seen 6 times to correct her pelvic position & posture, mainly left hip “ball & socket” restriction. “Stabilization exercises included bilateral hamstrings, gluteus maximus, adductors, and abdominals to maintain pelvic position/posture.” Conclusion: “The patient’s pain was eliminated 13 days after she first performed three exercises to reposition the pelvis and restore left posterior hip capsule extensibility and internal rotation…The patient no longer had numbness in her left leg, and sexual intercourse had become pain free.” Take Home Message: Six sessions and 13 days of an individualized corrective exercise program restored 10 months of SIJ-related hip pain. |
Mini SIJ Flexibility Self-Assessment
Here are the “normal” ranges of motion for 5 different checks that can be helpful for assessing SIJ dysfunction:
- Quadriceps length: Lying prone, heel should come close to touching your butt.

- Hamstring length: Lying supine, your straight leg should be able to get to 80-90°.

- Quadratus Lumborum length: Standing with feet together, sidebend to reach your hand down the side of your body. Fingers should reach the middle of the knee.

- Adductor Length: Lying supine, bent knees & feet together on the floor. Let both knees open to the outside, as if they would eventually touch the floor. Knee height from the floor should both be even, as well as nearer to the floor than up away from the floor.

- Pelvic Tilt: Standing, move your tail up and tail under a few times. See if you can determine which position of the tail is dominant (too far up or too far under). Your natural position should actually be “neutral” or balanced, without being locked into one or the other.
With the assessments above, feel free to stretch whichever areas do not have full range of motion, according to these norms. (And if you’d like a professional assessment, check out our 2-session online starter package here!)
Now, here are a few stretches that pelvic health physical therapists commonly prescribe for SIJ:
Child’s Pose Stretch
Why to do it: If you measured short in your Quadratus Lumborum / Standing Side Bend assessment above.
How to Do It: Kneel on the ground, splitting your knees apart enough for your body to settle down toward the floor, with your arms stretched out in front. If your left side is short, walk your hands over to the right, so that you feel a stretch in your left lower back area. (If both sides are short, then stretch both sides. If only one side is short, make sure to focus your stretch time on the side that is short.)
Hip swing “Stretch”
How to Do It: Stand near a stable support like a table or the back of a chair to hold onto for balance. Gently swing one leg forward and backward, allowing your hip to naturally move through a comfortable range of motion. Keep the movement controlled and smooth. The purpose is for you to let any hypomobile “stuck” SIJ to relax/release, using this form of decompression.
SI Joint-Friendly Tip: Do not force the leg to swing too high or too far back. Keep the motion within a pain-free range to avoid putting excessive strain on the SI joint. Maintain a slight bend in your standing hip, to practice activating the standing glute for natural balance. If this hurts either side, take this information to your corrective exercise specialist.
Figure 4 / Pigeon Pose / Hip External Rotators Stretch
When to Do It: When your external rotation assessment has shown that your hip external rotators do not have enough range of motion.
How to Do It:
- Seated on chair: Sit on a chair with your feet flat on the floor. Place your right ankle on your left knee, forming a “figure 4″. Gently lean forward, hinging from your hips, keeping your back straight, until you feel a stretch in the right hip and buttock. (Do both sides.)
- Laying on your back: Cross your right ankle onto your left knee, forming a “figure 4.” Clasp your hands around the back of your left thigh, to feel the stretch in your right hip area.
- Sitting on the floor: Place your left leg in front into a 90° position, and your right leg to the side, also in a 90° position. Let your body drop forward onto the left leg, feeling the stretch in your left hip. Do this stretch on whichever side has shortened Hip External Rotators.
SI Joint-Friendly Tip: With each exhale, engage your abdominal muscles to stabilize your spine and train your core stability.
Hip Internal Rotation Stretch
When to Do It: When your internal rotation assessment has shown that your hip internal rotators do not have enough range of motion.
How to Do It:
- Laying on your back: Bend both knees, leaving feet on the floor. To stretch your left hip internal rotators, walk your left foot out to the left just a few inches, and let your left knee fall inward. Place your right leg on top of your left knee, in a way that gently encourages the left leg to internally rotate. You must feel this in your hip, as it rotates inward, not in your lower back or your knee.
- Sitting on the floor: Place your left leg in front into a 90° position, and your right leg to the side, also in a 90° position. Let your hips turn toward the right leg, encouraging a stretch-sensation into the right hip rotators. Do this stretch on whichever side has shortened Hip Internal Rotators.
—————————–
If you would like fun & effective guidance during your own pregnancy, postpartum, or as a fitness professional, please check out these Fit For Birth offerings:
- Pregnancy, Pre-conception & Postpartum:
- Zoom virtual personal training – including our 2-session starter package specifically designed to give you a personal assessment, and most important corrective exercises!
- Online Pregnancy Program
- Fitness & Wellness Professionals:
—————————————————-
James Goodlatte is a Father, Holistic Health Coach, Corrective Exercise Practitioner, Speaker, Author, Professional Educator, and the founder of Fit For Birth. Since 2008, when he found out he would be a father, his passion for holistic wellness shifted to children and families. Today, he is a driving force in providing Continuing Education Credits for the pre and postnatal world, with Fit For Birth professionals in 52 countries. James is a contributing member of the First 1000 Days Initiative at the Global Wellness Institute, and longevity researcher & educator.
REFERENCES
[1] Image: Retrieved 2/8/24 from https://flowandgrowkidsyoga.com/blogs/news/flowing-through-cat-and-cow-poses
[2] 2010. McGill, Stuart. Core Training: Evidence translating to better performance and injury prevention. Strength and Conditioning Journal. Retrieved 2/8/25 from https://journals.lww.com/nsca-scj/fulltext/2010/06000/Core_Training__Evidence_Translating_to_Better.4.aspx?ref=popsugar.com&=___psv__p_46694987__t_w_
[3] Image: https://en.wikipedia.org/wiki/Sacroiliac_joint
[4] 2014. Bayer, Steve. SI Joint “Simplified”. PT Classroom. CyberPT. Retrieved 2/11/25 from https://www.cyberpt.com/sacroiliacjointsimplified.asp
[5] 2024. Alyson Powell Key. Medically reviewed by Jabeen Begum, MD. Sacroiliac Joint Dysfunction. WebMD. Retrieved 2/11/25 from https://www.webmd.com/back-pain/what-is-sacroiliac-joint-dysfunction
[6] 2008. Laslett, Mark.Evidence-based diagnosis and treatment of the painful sacroiliac joint. Journal of Manual & Manipulative Therapy. 16(3): 142–152. Retrieved 2/11/25 from https://pmc.ncbi.nlm.nih.gov/articles/PMC2582421/ AND http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2582421/
[7] 2024. Cocconi, et al. Sacroiliac joint pain: what treatment and when. Expert Review of Neurotherapeutics. Retrieved 2/11/25 from https://www.tandfonline.com/doi/abs/10.1080/14737175.2024.2400682
[8] 2019. Nejati, et al. Effectiveness of Exercise Therapy and Manipulation on Sacroiliac Joint Dysfunction: A Randomized Controlled Trial. Pain Physician Journal. Retrieved 2/11/25 from https://www.researchgate.net/profile/Parisa-Nejati/publication/331586497_Effectiveness_of_Exercise_Therapy_and_Manipulation_on_Sacroiliac_Joint_Dysfunction_A_Randomized_Controlled_Trial/links/62a1de70c660ab61f86fd254/Effectiveness-of-Exercise-Therapy-and-Manipulation-on-Sacroiliac-Joint-Dysfunction-A-Randomized-Controlled-Trial.pdf
[9] 2024. Trager, et al. Efficacy of manual therapy for sacroiliac joint pain syndrome: a systematic review and meta-analysis of randomized controlled trials. Journal of Manual & Manipulative Therapy. Retrieved 2/11/25 from https://www.tandfonline.com/doi/abs/10.1080/10669817.2024.2316420
[10] [2018] Weston, Carl. Practical Approaches to SI Joint Pain. Session #3302. Retrieved 2/11/25 from https://canfitpro.com/wp-content/uploads/2018/11/3302-Practical-Approaches-to-SI-Joint-Pain.pdf
[11] 2011. Boyle, Kyndall. Managing a Female Patient with Left Low Back Pain and Sacroiliac Joint Pain with Therapeutic Exercise: A Case Report. Physiotherapy Canada. Retrieved 2/11/25 from https://utppublishing.com/doi/abs/10.3138/ptc.2009-37