Understanding open vs closed glottis, and evidence-based outcomes for birth
For most women, childbirth delivery will be the most physically and mentally-emotionally demanding task of their lives. Having an understanding of breathing implications not only help during childbirth, but also allows prenatal fitness to be optimized.
Breathing during Life & Exercise
We will start our awareness of breathing during the pushing phase of labor by first looking at breathing during life & fitness.
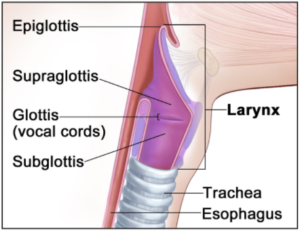
Glottis – the opening between the vocal folds in the larynx that is generally thought of as the primary valve between the lungs and the mouth[1]
Open vs Closed Glottis
Open glottis breathing allows air to pass freely in and out of the lungs without resistance. This type of breathing is what we would expect to occur naturally during the day, in activities such as resting, walking, or performing tasks that do not require intense physical exertion. However, due to the general stress and lack of fitness of much of the population, open glottis breathing is actually often not the baseline standard. (More on this in a moment.)
Closed glottis breathing occurs when air is momentarily trapped in the lungs by closing the glottis, typically during effort or strain. This is often unintentional during heavy lifts or strenuous parts of an exercise. In fact, people who have low core & stability function will inadvertently use closed glottis breathing for daily tasks as simple as opening a door or tying one’s shoelaces. This is because their body has recognized that these activities are actually “strenuous” enough to warrant a “desperate” attempt at max stabilization.
Glottis in Singing
In singing, the glottis plays a crucial role in producing sound, controlling pitch, and adding expressive qualities to the voice. When air passes through the glottis as the vocal cords vibrate, it generates sound. Singers learn to manipulate the tension and closure of the vocal cords to vary pitch and volume. Techniques like glottal stops, where the vocal cords briefly close completely before opening to let sound out, add articulation and emotion to singing.

Glottis in Fitness
In fitness, when a trainer asks you to breathe through an exercise, it is because he or she instinctively understands that if you are holding your breath, you are reinforcing the very same core & stability weakness that often leads to habitual closed-glottis breathing. Trainers are—in effect—asking you to try for more open glottis breathing.
How you breathe—open or closed glottis—can be a representation of your level of fitness. If you are already needing closed-glottis stability just for daily activities or “normal” strength training, it is a sign of poor function and low core stability. But if trainers can help you to use open glottis breathing for these lower level activities, then your body-mind can reserve the closed glottis breathing for those activities that are truly in need of it. Essentially, breathing through the exercise raises the bar for what your body can functionally handle. It makes you stronger, not necessarily today in this moment or during this rep, but for the rest of your life.
Intra-Abdominal Pressure (IAP) & Valsalva Maneuver
Open glottis breathing will generally create less intra-abdominal pressure (IAP). Higher IAP can be either good and bad, depending what your intention is.
- PRO: High IAP is often used intentionally during heavy weightlifting to stabilize the core and spine, enhancing the lifter’s ability to handle heavier loads.
- CON: While effective for stabilization, high IAP also significantly increases blood pressure and can pose risks,[2] especially for individuals with cardiovascular issues, or pelvic floor vulnerability, like during pregnancy & childbirth.
The Valsalva maneuver is a specific form of closed glottis breathing where an individual forcefully exhales against a closed airway, creating significant (higher) IAP. This is purposefully used during heavy strength training, especially with weights so heavy that they can only be lifted a few repetitions. The purpose is to create maximal stability for the extreme lift.
But best practices suggest that for most fitness activities, breathing should be open-glottis rhythmic and match the movement. For most people this needs to be a conscious practice while doing their fitness. Think of how you are often instructed to breathe during a yoga class. Your glottis is open, but your core is active, even as your breath moves rhythmically in and out. Moderate levels of IAP are able to be created to “core stabilize” during this kind of fitness breathing.
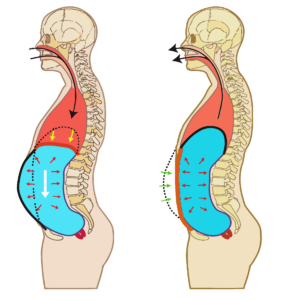
As such, it is recommended to use a controlled, open glottis diaphragmatic breathing technique for the majority of fitness activities. Diaphragmatic breathing means that you inhale into your entire torso, lower ribs and lower back, not just your chest and neck.
4 Stages of Breathing Progression During Exercise:
- Dysregulation of IAP: Poor breathing equates to poor core function, including poor IAP regulation. Since most people are poor breathers, dysregulation of IAP is the typical starting point for most untrained people. And it’s largely stemming from modern stressful and sedentary habits.
- Low to Moderate IAP should be generated naturally in many activities of daily life. This is also what fitness people can find themselves doing naturally, so long as their core-stability is functional (not always the case).
- It is better to generate mild IAP upon a foundation of Diaphragmatic Breathing. In this form of “core breathing” the inhalation is directed by the diaphragm, toward the lower torso. This is a better long-term practice than chest-breathing.
- Moderate to High IAP is generated from more Controlled Exhalations with Core Tightening: This is akin to Fit For Birth’s Core Breathing Belly Pump & can also be done with pursed lips to generate even more IAP.
- Highest IAP can be accomplished with the breath-holding Valsalva Maneuver, which is to be reserved for only the highest intensity strength training.

Stages of Labor: How to Breathe
Labor is typically divided into three main stages. For the vast majority of labor, the birthing person should be encouraged to breathe in whatever way she feels called to do! Understanding each stage will help inform expectant mothers and their support teams how to better breathe during the childbirth experience.
Stage 1: Latent & Active Labor (12-24 hours)
- Latent: As contractions begin, and gradually become stronger, the cervix will soften, thin, and open, up to 3-4 centimeters.
- Active: From 4 centimeters to the “full dilation” of 10 centimeters, contractions will typically occur about every 3-5 minutes. This is when she is likely to go to the birthing location, or ask her birthing attendants to come to her.
Stage 1 is a time for the laboring mom to be in her own meditative flow.
Stage 2: Pushing & Birth (few minutes to several hours)
This is the stage when mom feels a strong urge to push. While meditative flow remains key, many birthworkers will begin suggesting how to breathe during this pushing stage.
- In open-glottis pushing, the mother is encouraged to push when she feels the urge during a contraction, without holding her breath. This method involves exhaling or making noise through the mouth while pushing, keeping the glottis open.
- Closed-glottis pushing involves taking a deep breath at the start of a contraction, holding that breath, and then pushing down hard while keeping the mouth and glottis closed. This method is often compared to the effort of trying to have a bowel movement.
Which method is best? We will answer this question in the research below!
Stage 3: Delivery of the Placenta
Following the birth of the baby, the third stage involves the delivery of the placenta. Contractions will continue but are generally less intense, helping to separate the placenta from the uterine wall. The mother may be asked to push gently to help expel the placenta, usually within 5 to 30 minutes after the baby is born.

Research Study Conclusions on Breathing Methods during Labor
In order to answer the question, “What breathing method is best for childbirth pushing?”, we will examine the findings of several studies. We have consolidated the findings in this chart, and you can see more specifics of each study below that.
Research Summary Chart
| Glottis Study | C-section vs vaginal birth | Maternal outcomes | Neonatal outcomes | PF & perineal damage |
| 2016 Literature Review | No difference | N/A | Open glottis: healthier Apgar & pH | No difference |
| 2022 Maternal & Baby Outcomes | N/A | Open glottis: no need for oxygen & shortened 2nd stage labor | Open glottis: fewer babies sent to ICU | N/A |
| 2023 Perineal Trauma Quick-look | N/A | N/A | N/A | Open glottis: may cause less perineum damage |
| 2023 Operative Vaginal Delivery | No difference in 1st time labors. |
For 2nd time laborers, open glottis reduced operative vaginal rates.No difference No differenceN/A2023 Regulated Expiration DeviceNot a significant differenceFocused breathing: Shortened labor duration & reduced pain N/AN/A
2016 Glottis Literature Review [3]
A literature review is awesome because it gives an overview of a whole bunch of prior studies, intending to quickly get us up to speed on previous findings. This 2016 review covered seven studies using pertinent keywords from 1980 to 2015! Regarding open and closed glottis breathing techniques, authors of this literature review found:
- No differences for perineal injuries
- No differences for episiotomies
- No differences in type of birth (vaginal vs c-section)
- One study found that open-glottis users had babies with better 5-minute Apgar scores and better umbilical artery pH.
2022 Glottis Breathing on Maternal & Baby Outcomes [4]
This study was performed on 150 Egyptian women who are giving birth for the first time. Half used open glottis breathing, and the other half used closed glottis breathing during pushing.
Their conclusions were that open glottis pushing during 2nd stage labor:
- Enhanced neonatal and maternal outcomes, as indicated by these results:
- “Oxygen wasn’t used at all” in the open glottis pushing (compared to 74% in the closed glottis group).
- “In the closed glottis pushing group, a higher proportion of babies are admitted to ICU than those in the open glottis pushing group (18.0 percent versus 10.0 percent).”
- Shortened 2nd stage labor by 5-10 minutes.
2023 Perineal Trauma Quick Look [5]
An informal review found that in first time birthing moms, open glottis breathing may produce a generally higher frequency of intact perineum, and reduction in long tears.
2023 Glottis Breathing for Operative Vaginal Delivery[6]
More than 3000 French women were studied, with 19% using open glottis pushing and 81% using closed glottis pushing. Creators of this study primarily wanted to determine the likelihood of “operative vaginal delivery” which means births in which instruments are used to assist in the delivery of a baby vaginally. Operative vaginal deliveries typically involve the use of forceps or a vacuum https://entrance.kathmandu.gov.np/Scholarship/ device (vacuum extraction) to help guide the baby out of the birth canal. This type of delivery is employed when a vaginal delivery is considered preferable but the mother is unable to push the baby out on her own due to fatigue, distress, or other complications, or if the baby needs to be delivered more quickly than can be achieved by pushing alone.
The conclusion in this study was that the risk of operative vaginal birth did not differ according to the glottis mode of pushing for women who have never before given birth, and who are delivering only one baby. However, amongst women who have given birth to one or more children, the operative vaginal delivery rate was significantly lower when using open- compared with closed-glottis pushing.
Regardless of the number of children delivered or not, other maternal and neonatal outcomes did not differ between the 2 modes of glottis pushing.
2023 Regulated Expiratory Method (REM)[7]
In this study, 120 first time Canadian birthing women were randomized into two groups, primarily to determine if a particular breathing device could affect cesarean rates. The conclusion was: “Despite no significant reduction in immediate cesarean rates, REM has the potential, as a non-pharmacological approach, to shorten labor duration, pain management, and ultimately improve maternal childbirth experience.”
Specific results found that this focused breathing device:
- Reduced c-section to 18.3% (from 26.7%, but this change was not deemed to be “significant”)
- Significantly reduced Stage 2 labor and pushing effort times.
- Facilitated communication between midwives and birthing mothers.
- Had a significant positive impact on the mothers childbirth experience.
According to the research study, REM is a technique that allows for the activation of the abdominal muscles without generating High IAP, achieved through the resistance to expiration provided by the mouthpiece. The primary function of the device is to control the speed and pressure of air being exhaled.
The device was used during both the 1st and 2nd stages of labor. During the pushing phase, a deep inhalation at the start of a contraction was followed by a naturally accompanying contraction of both the abdominal and uterine muscles. The study authors explained that the IAP does rise, and does direct the force toward the pelvic floor (PF). Authors believe that using this device “protects the perineum from excessive pressure.” In comparison to the typical closed-glottis breathing technique, this statement is true, but not necessarily in comparison to open glottis breathing during labor. Authors, however, also believed that open glottis pushing is more challenging for people to do.
Authors also stated, “In this study, constantly exhaling into the mouthpiece enabled patients to regain control of their pain, breathing and pushing efforts. Patients were more often calm with easier communication with their midwives.”

What Breathing Method is Best for Pushing During Labor?
According to multiple scientific studies, open glottis breathing has variously been associated with healthier babies, better maternal outcomes, and the possibility of less damage to the pelvic floor (PF) areas, although these outcomes have not necessarily been repeated consistently. Meanwhile, focused core breathing which regulates intra-abdominal pressure (IAP) may also provide some maternal benefits.
- Closed glottis “breath holding” causes PF pressure. Closed glottis, or Valsalva, breathing absolutely puts more pressure on the PF. This could result in damage from too forceful a generation of IAP that puts pressure on already weakened PF areas.
- Open glottis breathing has naturally lower IAP, and therefore puts less pressure on PF structures, muscles, perineum, etc. However, if this pressure is not enough to progress the pushing stage of labor, hospital staff may elect for interventions to try to get labor to progress faster.
Breathing devices designed to restrict exhalation may be able to produce a nice balance between the two styles of open and closed glottis breathing. The same effect can be accomplished using traditional fitness’ pursed lips exhalation. This form of pursed-lips “core breathing” activates important abdominal muscles while simultaneously creating a moderate IAP (not too high to cause damage, nor too low to prevent progress).
For more than a decade, Fit For Birth clients have regularly reported how the open-glottis core-activated Core Breathing Belly Pump (CBBP) helped them push their babies less than 20 minutes, sometimes in just a few pushes. Adding pursed lips to the CBBP is an ideal framework for Fit For Birth practitioners to coach their clients.
————————————————————————
If you would like fun guidance during your own pregnancy, postpartum, or as a fitness professional, please check out these Fit For Birth offerings:
- Pregnancy & Postpartum:
- Pregnancy & Pre-conception: Online Pregnancy Wellness Course
- Fitness & Wellness Professionals:
—————————————————-
James Goodlatte is a Father, Holistic Health Coach, Corrective Exercise Practitioner, Speaker, Author, Professional Educator, and the founder of Fit For Birth. Since 2008, when he found out he would be a father, his passion for holistic wellness shifted to children and families. Today, he is a driving force in providing Continuing Education Credits for the pre and postnatal world, with Fit For Birth professionals in 52 countries. James is also the program director for Fit For Birth pre & postnatal personal training worldwide, and is a contributing member of the First 1000 Days Initiative at the Global Wellness Institute.
[1] 2006. J.H. Esling. Encyclopedia of Language & Linguistics (Second Edition). Retrieved 2/8/24 from https://www.sciencedirect.com/topics/medicine-and-dentistry/glottis
[2] 2018. Nall, Rachel. What is the Valsalva maneuver? Medical News Today. Retrieved 2/8/24 from https://www.medicalnewstoday.com/articles/322661#uses
[3] 2016. Barasinski, et al. Do maternal pushing techniques during labour affect obstetric or neonatal outcomes? Gynécologie Obstétrique & Fertilité. Retrieved 2/6/24 from https://www.sciencedirect.com/science/article/abs/pii/S1297958916301801
[4] 2022. Mohamed et al. Egyptian Journal of Health Care. Effect of Open Glottis versus closed Glottis (Valsalva) in Second Stage of Labor on Maternal andNeonatal Outcomes. Retrieved 2/6/24 from https://ejhc.journals.ekb.eg/article_226064_bf4b7b667c69bf2c1dc0962c6541d831.pdf
[5] 2023. De Souza Santos Sachs, et al. Open Glottis During Delivery and Perineal Trauma. American Family Physician. Retrieved 2/7/24 from https://www.aafp.org/pubs/afp/issues/2023/0800/fpin-ci-open-glottis-perineal-trauma.html
[6] 2023. Froeliger, et al. AMerican Journal of Obstetrics and Gynecology. Closed- or open-glottis pushing for vaginal delivery: a planned secondary analysis of the TRAnexamic Acid for Preventing postpartum hemorrhage after vaginal delivery study. Retrieved 4/17/24 from https://pubmed.ncbi.nlm.nih.gov/37633725/
[7] 2023. Dimassi, et al. Regulated Expiratory Methods During Childbirth Process: A Randomized Controlled Trial. Journal of Obstetrics and Gynaecology Canada. [Rented]. Retrieved 2/6/24 from https://www.sciencedirect.com/science/article/abs/pii/S170121632300628X