
Research-based and updated on September 24, 2021
If you haven’t yet read the first portion of this informational series, “What Happens to the Abdominal Muscles During a C-Section”, consider visiting that article first. That article shows that abdominal muscles do indeed get cut during a c-section. This article will show specific kind of cuts, usual practices & procedures of C-section, and videos in the operating room.
Historical Background
“The first documented cesarean delivery (CD) was in 1020 AD. In 1882, the era of modern CD began when Saenger advocated closing all uterine incisions immediately after surgery. The lower uterine segment incision was introduced by Kronig in 1912 and popularized in the United States by DeLee in 1922. The transverse uterine incision was described by Munro-Kerr in 1926…Approximately 2 CDs are started every minute in the United States alone; this is the most frequent major operation that is performed in this country.”1
Overview of the Tissues that Get Cut during a C-Section
How many layers are cut?!
Various references include various “numbers” of layers that are cut. Though this is a common web search query, it will not yield identical results every time because some layers of fascia are counted together in some references, while separated in other references. (For example, one could say – simplistically – that there are just 3 layers that are cut during a C-section: Skin, abdominal wall fascia, and then uterus. Some references use the number 7: skin, fat, fascia, muscles, more fascia, uterus, amniotic sac.2)
However many layers get cut, the reality is that, “to achieve a cesarean delivery, the surgeon must traverse all the layers that separate him/her from the fetus,”3 which absolutely include all fascia connected to the abdominal muscles. Here is one description that uses 4 layers.4
1. “First, the skin is incised, followed by the subcutaneous tissues.”
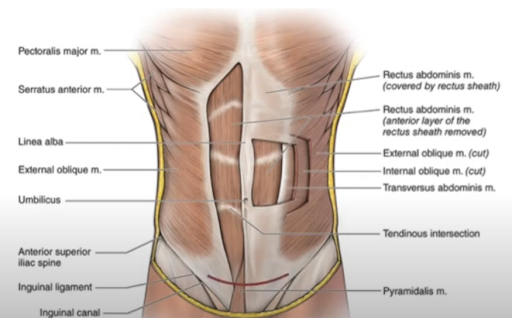
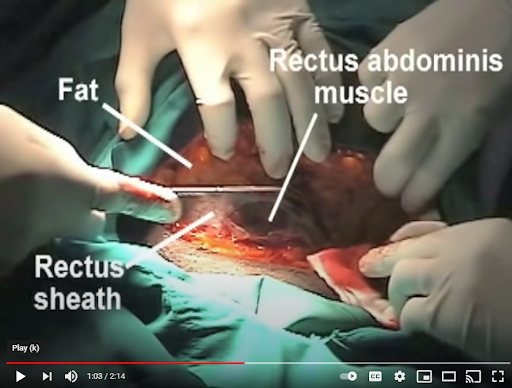
2. “The next layer is the fascia overlying the rectus abdominis muscles. The anterior abdominal fascia usually consists of two layers. One is composed of the aponeurosis from the external oblique rectus muscle, and the other is a fused layer which contains the aponeuroses of the transverse abdominis and internal oblique muscles.”
- Fascia – a thin sheath of fibrous tissue enclosing a muscle or other organ
- Aponeurosis – a sheet of fibrous tissue that takes the place of a tendon in flat muscles having a wide area of attachment
3. “After separating the rectus muscles…the surgeon enters the abdominal cavity through the parietal peritoneum.”
- Peritoneum – membrane lining the cavity of the abdomen and covering the abdominal organs
4. “Depending on the status of the patient’s amniotic membranes (if her “water is broken” or intact), the surgeon could encounter that amniotic sac upon incision of the uterus…The amniotic sac, if present, would be the last layer between the surgeon and the fetus. It is at this point that the fetus is delivered, achieving the primary goal of the cesarean section.”
According to 2010 research in Gynecological Surgery, “At the most basic level, the only thing necessary is some cutting instrument. In an emergency, a physician could theoretically perform a perimortem cesarean delivery on a woman after a car accident with a sharp piece of glass.”5 Equipment used can include: catheter running from the bladder, regional or general anesthesia, and a surgical tray that includes scissors, bandages, clamps, forceps, retractors, needle drivers and more.
The four main cesarean delivery techniques are6:
- Pfannenstiel-Kerr – Pfannenstiel skin incision, followed by multiple sharp dissections (not blunt), closure of peritoneum, interrupted fascia closure, continuous skin suture.
- Joel-Cohen – JC skin incision, followed by multiple blunt dissections, spontaneous placenta removal, non-closure of peritoneum
- Misgav-Ladach – Same as JC (JC skin incision and blunt dissections), except: Misgav-Ladach uses manual placenta removal (not spontaneous), single layer running closure of the uterus (not interrupted), continuous closure of the fascia (not interrupted), mattress closure of the skin (not continuous)
- Modified Misgav-Ladach – Pfannenstiel skin incision, followed by multiple blunt dissections, spontaneous placental removal, running uterine closure (not interrupted), closure of the peritoneum, continuous closure fascia closure, continuous skin suture.
Explanation of Closure/Sutures:
- Continuous/Running = single thread
- Interrupted = multiple small threads, one after the other

Details of Basic C-section steps7:
We wrote our first article, “What Happens to the Abdominal Muscles during a C-Section” specifically to dispel the myth that many of our client’s hear from their medical staff: “that no muscles are cut.” This is dangerously misleading because it infers that recovery is not such a big deal. Statements like these are aligned with the common medical agenda to do what they are most well-trained for: administering drugs and performing surgery. That first article was originally titled, “What Muscles Get Cut During a C-Section?” in hopes to help educate our clients to understand what they may be signing up for.
The reality is that clients who undergo a C-section are grossly neglected, unlike most other “major surgeries.” As a classified “major surgery” C-section is on par with other surgeries like hip replacements. Yet, there is no standardized rehabilitation protocol for a C-section. Although this is the current state of modern hospital birthing, it is not acceptable, and needs to improve. That first step of change is awareness.
So here is an overview of exactly how the various steps & layers of the abdominal wall are cut and moved, in order to pull a fetus out during a C-section.
1. “A Pfannenstiel skin incision is slightly curved and is located 2 to 3 centimeters or 2 fingerbreadths above the symphysis pubis. The midportion of the incision is within the hair-bearing area of the mons. The hair should be removed in this case. A Joel-Cohen incision, in contrast, is straight rather than curved. It is 3 cm below the line connecting the anterior superior iliac spines, making it more cephalad than a Pfannenstiel skin incision”
2. The subcutaneous layer is next, and it can be dissected bluntly or sharply.
3. “The fascia is then incised in the midline with the scalpel, and this incision is extended laterally either sharply or bluntly.”
4. “After separating the rectus muscles in the midline, entry into the abdominal cavity is achieved through opening the peritoneum.”
5. “Upon achieving uterine entry, the uterine incision can be extended laterally either bluntly with fingers or sharply with bandage scissors.” (Hysterotomy is incision in the uterus)
6. “The peritoneum can be reapproximated at this time. Closure of the peritoneum adds operative time, and it may increase postoperative fever and length of hospital stay. The decision to close this layer often hinges on the surgeon’s interpretation of the literature regarding whether closure decreases adhesion formation. Unfortunately, this data is mixed, and therefore, it is the surgeon’s prerogative to balance the risks and benefits to the patient.”
7. “Before the closure of the fascia, the rectus muscles and the subfascial tissues are inspected to ensure hemostasis. The rectus muscles can be reapproximated in advance of fascial closure. Some surgeons believe that suturing the muscles reduces the risk of subsequent diastasis recti and decreases the incidence of intra-abdominal adhesion formation. Conversely, reapproximating the muscles leads to increased postoperative pain. Given time, the surgeon could involve the patient herself in shared decision making regarding this technique.”
8. “The fascia is then closed using delayed-absorbable suture in a running nonlocking fashion. Historically, the fascia has been closed by some in an interrupted fashion, but this technique is no longer widely used.”
9. “Skin closure may be accomplished using a variety of methods, the most common being surgical staples or subcuticular suture.”
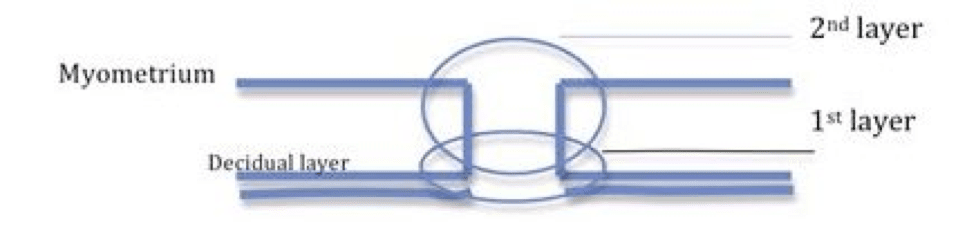
Overview of Cesarean Closure after baby is delivered16:
- 1. First layer of Uterus: “the first layer of suture (the endometrial layer) can be either a simple running suture or a running locked suture. The locked suture is more hemostatic and is used especially when there is evidence of arterial bleeding.”
- 2. Second layer of Uterus: “this overlaying layer (through the myometrium) should hide the first layer beneath it when it is closed. This is typically a simple running suture.”
- 3. “Fascia closure: the peritoneum layers and the rectus muscle are not usually closed. Instead the closing of the rectus fascia provides most of the wounds strength for the abdominal incision. This is often a simple running suture/continuous suture.”
- 4. “Closing of the skin: is the last step. A subcuticular suture method is used to minimize the scar that will remain from the procedure.
Should Abdominal Muscles be Closed During a C-section to Address Diastasis Recti?
According to 2010 research in Gynecological Surgery, “Reapproximation of rectus muscle seems to be unnecessary also because the muscles tend to find the right anatomic location by itself. For this reason and because it may produce unnecessary pain when the woman starts to move after the operation, suturing it is not recommended. There are no published data to support or refuse these claims. Further studies are needed.”17
While it is wonderful that the rectus abdominis muscles tend to find their correct anatomical position, it is altogether another question as to whether or not abdominal wall function returns, as well as whether or not the patient feels that her aesthetics and comfort return as well.
Addressing your client’s function after a diastasis recti and C-section is absolutely critical. It is the most important of the 6 crucial elements for treating diastasis.
————————————————————————————————————————————-
Videos Helping To Understand C-Section, Layer by Layer
Overview of this AUAUniversity Video:
Pfannenstiel incision is a low transverse, semi circular incision
Benefits:
- Cosmetic (well-hidden)
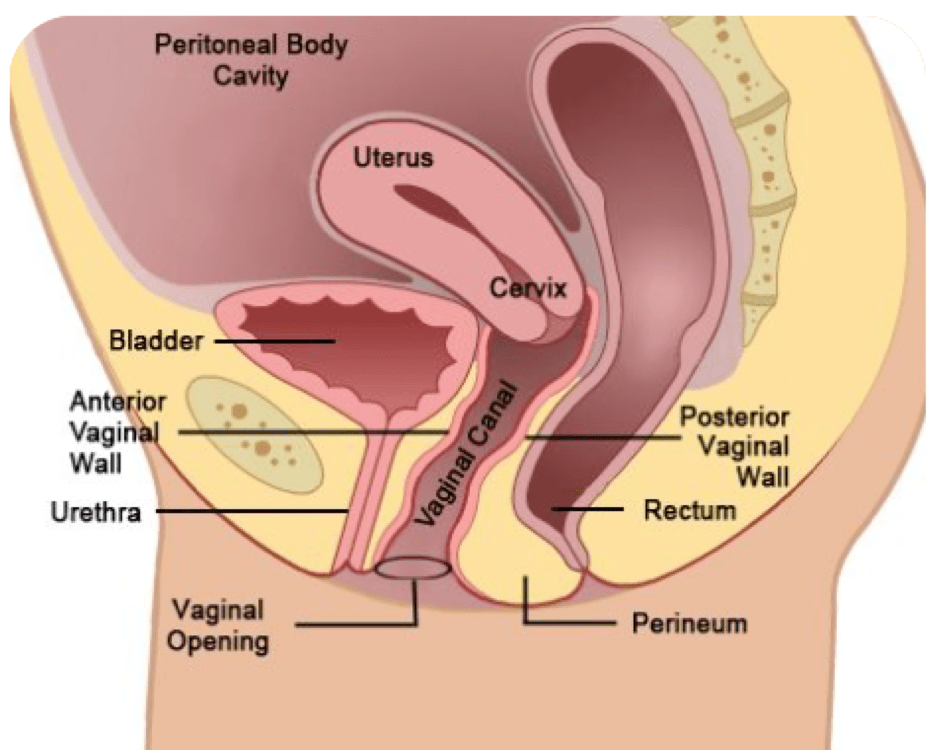
- Excellent access to: retropubic space, bladder, ureters
- The retropubic space (also known as the prevesical space, cave of Retzius or cavum Retzii) is an extraperitoneal space located posterior to the pubic symphysis and anterior to the urinary bladder. It is separated from the anterior abdominal wall by the transversalis fascia and extends to the level of the umbilicus.”19
- “The extraperitoneal space is the portion of the abdomen and pelvis which does not lie within [the] peritoneum.20
- “The peritoneum is a continuous membrane which lines the abdominal cavity and covers the abdominal organs (abdominal viscera). It acts to support the viscera, and provides pathways for blood vessels and lymph to travel to and from the viscera.”21
- The peritoneum includes:22
- Retroperitoneal space, situated posteriorly to the peritoneum.
- Preperitoneal space, situated anteriorly to the peritoneum
- Retropubic space, deep to the pubic bone
- Retro-inguinal space, deep to the inguinal ligament”
- Remain extra-peritoneal with option of intraperitoneal entry with superior extension”
- “The extraperitoneal space is the portion of the abdomen and pelvis which does not lie within [the] peritoneum.20
- The retropubic space (also known as the prevesical space, cave of Retzius or cavum Retzii) is an extraperitoneal space located posterior to the pubic symphysis and anterior to the urinary bladder. It is separated from the anterior abdominal wall by the transversalis fascia and extends to the level of the umbilicus.”19
AUAUniversity Video Continued:
The anatomy that will be visualized in this type of incision, proceeding from superficial to deep, will be the:
- 1 – Skin
- 2 – Camper’s Fascia
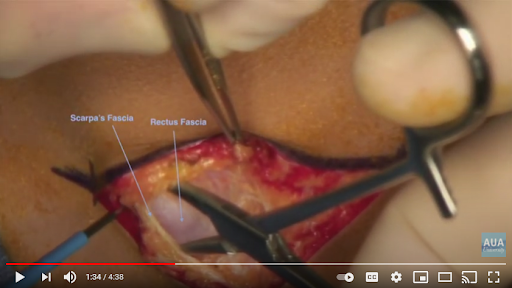
- 3 – Scarpa’s Fascia
- 4 – Rectus Fascia
- The rectus sheath, also called the rectus fascia, is formed by the aponeuroses of the transverse abdominal and the internal and external oblique muscles. It contains the rectus abdominis and pyramidalis muscles.”24
- “Aponeurosis, a flat sheet or ribbon of tendonlike material that anchors a muscle or connects it with the part that the muscle moves.”
- The aponeurosis (sheet-like fibrous tendon) of three flat muscles (EO, IO, TVA) “become entwined, forming the linea alba.”
- The rectus sheath, also called the rectus fascia, is formed by the aponeuroses of the transverse abdominal and the internal and external oblique muscles. It contains the rectus abdominis and pyramidalis muscles.”24
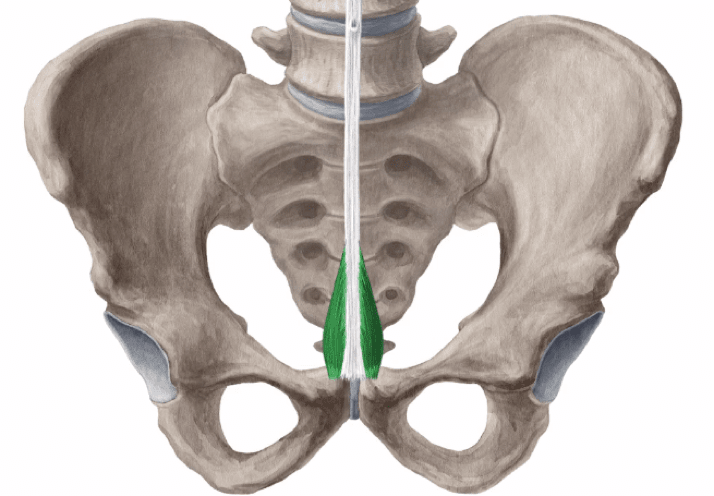
- 5 – Pyramidalis Muscle
- FUNCTION:
- “Pyramidalis muscle tenses the linea alba, which is an action that doesn’t have a significant function when occurring on its own. However, acting together with the rest of the abdominal muscles, pyramidalis muscle contributes to a variety of abdominal wall functions, such as increasing the intra abdominal pressure when necessary (e.g. labor, forced expiration, defecation).”25
- 2020 Research Study: “It is believed that the pyramidalis muscle’s function is to strengthen the abdominal wall and tense the linea alba. However, its absence does not cause apparent loss of function. Hence, despite the aforementioned extensive description, the pyramidalis muscle’s function is still unclear. Because of that, some authors consider it a vestigial muscle, leftover from the marsupials’ and monotremes’ pouch, evolving into an irregular apparition in more evolved primates, often observed in chimpanzees and gorillas but absent in orangutans. There are also anthropological studies suggesting that the pyramidalis has evolved as part of the normal human anatomy, in which case it could be related to the species’ erect posture.”26
- “Pyramidalis is classified as a vestigial muscle which is frequently present. It is [a] muscle of the anterior abdominal wall. It is thought to tense the linea alba. It has been used as a surgical landmark, source of muscle stem cells https://moratuwa.mc.gov.lk/ and in various surgical procedures…Many authors have related the pyramidalis muscle with erection of the penis or assumption of upright posture in humans.”27
- “Vestigial muscles in human beings are those muscles which are tendinous in larger part or reduced in size compared to the homologous muscles in other species or is frequently absent within or between populations…Phylogenetically, pyramidalis is linked to the pouch inside monotremes such as hedgehog and the platypus and marsupials such as the koala or kangaroo.”28
- FUNCTION:
- 2017 Cadaver Study on Indian Population30: “The pyramidalis muscle was present in 92% [Indian] cases, usually bilaterally (72%) than unilaterally (20%) and more frequently in males (94.11%) than in females (87.5%)…In Japanese population, the incidence of pyramidalis was greater (94.5%) as compared to our study population. Incidence in the present study was greater than that reported in American blacks (82%)….It varies considerably in size and may be larger on one side than on the other, sometimes absent on one or both sides, or occasionally doubled. The incidence of this muscle also varies greatly with sex and race….”
- 6 – Linea Alba of Rectus Muscle
- 7 – Transversalis Fascia
- The transversalis fascia is a thin aponeurotic membrane which lies between the inner surface of the Transversus and the extraperitoneal fat. It forms part of the general layer of fascia lining the abdominal parietes, and is directly continuous with the iliac and pelvic fasciae.”33
- TVA Muscle’s: “upper three-fourths lie behind the rectus muscle and blend with the posterior lamella of the aponeurosis of the internal oblique; its lower fourth is in front of the rectus abdominis.”34
- [Transversalis Fascia can be considered a tendon of the TVA]
- 8 – Pre-Vesical Fat
- 9 – Bladder
- 10 – Peritoneum (superiorly)
“The Arcuate Line, or Semicircular line of Douglas is located roughly one-third of the distance from the pubic crest to the umbilicus. It is the demarcation where the internal oblique and transversus abdominis aponeuroses of the rectus sheath start to pass anteriorly to the rectus abdominis muscle, leaving only the transversalis fascia posteriorly.”35

—————————–
If you would like clarifying, research-based guidance as a fitness professional – during your own pregnancy, postpartum – please check out these Fit For Birth offerings:
- Fitness & Wellness Professionals:
- FREE 2-hour CEC
- All CEC/CEU Courses – Including our Pre & Postnatal Diastasis and Core Consultant Course (PPDCC), which provides step-by-step instructions on how to rehabilitate your clients who have C-section.
- Monthly Elite Membership
- Pregnancy, Pre-conception & Postpartum:
—————————————————-
James Goodlatte is a Father, Holistic Health Coach, Corrective Exercise Practitioner, Speaker, Author, Professional Educator, and the founder of Fit For Birth and Exercise For Longevity. Since 2008, when he discovered that he would be a father, his passion for holistic wellness shifted to children and families. Today, he is a driving force in providing Continuing Education Credits for the pre and postnatal world, with Fit For Birth professionals in 52 countries. James is a contributing member of the First 1000 Days Initiative at the Global Wellness Institute, and longevity researcher & educator.
References
- Berghella, et al. Evidence-based surgery for cesarean delivery. American Journal of Obstetrics & Gynecology. Retrieved 4/21/21 from https://www.ajog.org/article/S0002-9378(05)00500-4/fulltext ↩︎
- [n.d.] You’ve had a C-section – now what? Carolina Pelvic Health Center, Inc. Retrieved 9/24/24 from https://carolinapelvichealth.com/c-section-birth-your-guide-to-recovery/#:~:text=A%20C%2Dsection%20includes%207,and%20finally%20the%20amniotic%20sac. ↩︎
- 2023. Sung, Sharon. Mahdy, Heba. Cesarean Section. StatPearls [Internet]. Retrieved 8/21/24 from https://www.ncbi.nlm.nih.gov/books/NBK546707/ ↩︎
- 2023. Sung, Sharon. Mahdy, Heba. Cesarean Section. StatPearls [Internet]. Retrieved 8/21/24 from https://www.ncbi.nlm.nih.gov/books/NBK546707/ ↩︎
- 2023. Sung, Sharon. Mahdy, Heba. Cesarean Section. StatPearls [Internet]. Retrieved 8/21/24 from https://www.ncbi.nlm.nih.gov/books/NBK546707/ ↩︎
- 2023. Sung, Sharon. Mahdy, Heba. Cesarean Section. StatPearls [Internet]. Retrieved 8/21/24 from https://www.ncbi.nlm.nih.gov/books/NBK546707/ ↩︎
- 2023. Sung, Sharon. Mahdy, Heba. Cesarean Section. StatPearls [Internet]. Retrieved 8/21/24 from https://www.ncbi.nlm.nih.gov/books/NBK546707/ ↩︎
- 2010. Bolla, et al. Technical aspects of the cesarean section. Gynecological Surgery. Retrieved 4/21/21 from https://gynecolsurg.springeropen.com/articles/10.1007/s10397-010-0560-9 ↩︎
- 2010. Bolla, et al. Technical aspects of the cesarean section. Gynecological Surgery. Retrieved 4/21/21 from https://gynecolsurg.springeropen.com/articles/10.1007/s10397-010-0560-9 ↩︎
- 2010. Bolla, et al. Technical aspects of the cesarean section. Gynecological Surgery. Retrieved 4/21/21 from https://gynecolsurg.springeropen.com/articles/10.1007/s10397-010-0560-9 ↩︎
- 2015. Gizzo, et al. Caesarean Section: Could Different Transverse Abdominal Incision Techniques Influence Postpartum Pain and Subsequent Quality of Life? A Systematic Review. PLOS ONE. Retrieved 4/21/21 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4315586/ ↩︎
- 2010. Bolla, et al. Technical aspects of the cesarean section. Gynecological Surgery. Retrieved 4/21/21 from https://gynecolsurg.springeropen.com/articles/10.1007/s10397-010-0560-9
↩︎ - 2023. Sung, Sharon. Mahdy, Heba. Cesarean Section. StatPearls [Internet]. Retrieved 8/21/24 from https://www.ncbi.nlm.nih.gov/books/NBK546707/ ↩︎
- 2016. Cesarean Section/Cesarean Delivery. Stepwards. Retrieved 4/21/21 from https://www.stepwards.com/?page_id=3610 ↩︎
- 2016. Cesarean Section/Cesarean Delivery. Stepwards. Retrieved 4/21/21 from https://www.stepwards.com/?page_id=3610 ↩︎
- 2016. Cesarean Section/Cesarean Delivery. Stepwards. Retrieved 4/21/21 from https://www.stepwards.com/?page_id=3610 ↩︎
- 2010. Bolla, et al. Technical aspects of the cesarean section. Gynecological Surgery. Retrieved 4/21/21 from https://gynecolsurg.springeropen.com/articles/10.1007/s10397-010-0560-9 ↩︎
- 2020. AUAUniversity. Core Videos (2019): Open Surgical Approaches: Pfannenstiel Incision. YouTube. Retrieved 4/21/21 from https://www.youtube.com/watch?v=Yma-72HE0NA ↩︎
- 2021. Melbourne Uni Radiology Masters. Retropubic Space. Radiopaedia. Retrieved 9/24/21 from https://radiopaedia.org/articles/retropubic-space?lang=us#:~:text=The%20retropubic%20space%20(also%20known,the%20level%20of%20the%20umbilicus. ↩︎
- [n.d.] Micheau, Antoine. Extraperitoneal space. e-Anatomy at IMAIOS. Retrieved 9/24/24 from https://www.imaios.com/en/e-Anatomy/Anatomical-Parts/Extraperitoneal-space#:~:text=The%20extraperitoneal%20space%20is%20the,situated%20posteriorly%20to%20the%20peritoneum ↩︎
- 2024. O’Neill, Katie. The Peritoneum. TeachMeAnatomy. Retrieved 9/24/24 from https://teachmeanatomy.info/abdomen/areas/peritoneum/#:~:text=The%20peritoneum%20is%20a%20continuous,to%20and%20from%20the%20viscera.
↩︎ - [n.d.] Micheau, Antoine. Extraperitoneal space. e-Anatomy at IMAIOS. Retrieved 9/24/24 from https://www.imaios.com/en/e-Anatomy/Anatomical-Parts/Extraperitoneal-space ↩︎
- 2019. AUAUniversity. Core Videos (2019): Open Surgical Approaches: Pfannenstiel Incision. YouTube. Retrieved 8/21/21 from https://www.youtube.com/watch?v=Yma-72HE0NA ↩︎
- [n.d.] Rectus Sheath. Wikipedia. Retrieved 4/21/21 from https://en.wikipedia.org/wiki/Rectus_sheath ↩︎
- 2023. Vaskovic, Jana, MD. McLaren, Nicola, MSc. Pyramidalis muscle. KenHub. Retrieved 4/21/21 from https://www.kenhub.com/en/library/anatomy/pyramidalis-muscle
↩︎ - 2020. Hojaij, et al. Morphometry and Frequency of the Pyramidalis Muscle in Adult Humans: A Pyramidalis Muscle’s Anatomical Analysis. Clinics. Retrieved 4/21/21 from https://www.scielo.br/pdf/clin/v75/1807-5932-clin-75-e1623.pdf
↩︎ - 2017. Swaroop Das, et al. Biometrics of Pyramidalis Muscle and its Clinical Importance. Journal of Clinical & Diagnostic Research. Retrieved 4/21/21 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5376864/#:~:text=Pyramidalis%20is%20classified%20as%20a,and%20in%20various%20surgical%20procedures. ↩︎
- 2017. Swaroop Das, et al. Biometrics of Pyramidalis Muscle and its Clinical Importance. Journal of Clinical & Diagnostic Research. Retrieved 4/21/21 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5376864/#:~:text=Pyramidalis%20is%20classified%20as%20a,and%20in%20various%20surgical%20procedures. ↩︎
- Image: 2023. Vaskovic, Jana, MD. McLaren, Nicola, MSc. Pyramidalis muscle. KenHub. Retrieved 4/21/21 from https://www.kenhub.com/en/library/anatomy/pyramidalis-muscle
↩︎ - 2017. Swaroop Das, et al. Biometrics of Pyramidalis Muscle and its Clinical Importance. Journal of Clinical & Diagnostic Research. Retrieved 4/21/21 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5376864/#:~:text=Pyramidalis%20is%20classified%20as%20a,and%20in%20various%20surgical%20procedures.
↩︎ - 2015. Natsis, et al. Morphometric variability of pyramidalis muscle and its clinical significance. Surgical and Radiologic Anatomy. Springer Link. Retrieved 9/24/24 from https://link.springer.com/article/10.1007/s00276-015-1550-4
↩︎ - 2020. Hojaij, et al. Morphometry and Frequency of the Pyramidalis Muscle in Adult Humans: A Pyramidalis Muscle’s Anatomical Analysis. Clinics. Retrieved 4/21/21 from https://www.scielo.br/pdf/clin/v75/1807-5932-clin-75-e1623.pdf
↩︎ - [n.d.] Transversalis fascia. e-Anatomy at IMAIOS. Retrieved 9/24/24 from https://www.imaios.com/en/e-Anatomy/Anatomical-Parts/Transversalis-fascia ↩︎
- [n.d.] Transverse abdominal muscle. Wikipedia. Retrieved 9/24/24 from https://en.wikipedia.org/wiki/Transverse_abdominal_muscle ↩︎
- 2023. Yu, Yoshi. Arcuate Line. Radiopaedia. Retrieved 9/24/24 from https://radiopaedia.org/articles/arcuate-line?lang=us ↩︎
- 2013. Openmichigan. Caesarean Section: Step 2 – Abdominal Incision. YouTube. Retrieved 9/24/24 from https://www.youtube.com/watch?v=lMQLE7Ruk0Q ↩︎
- 2010. Drkapilkishore. Cesarean birth / C Section / LSCS/ Child Birth. YouTube. Retrieved 9/24/24 from https://www.youtube.com/watch?v=gJeRWGxOTcA ↩︎
- 2020. Dr Rahul Jadhao. Misgav Ladach technique of caesarean section -Dr Rahul Jadhao. YouTube. Retrieved 9/24/24 from https://www.youtube.com/watch?v=U8lARiRmV3E ↩︎
- 2012. Hammydude12345. Cesarean Section Operative Technique. YouTube. Retrieved 9/24/24 from https://www.youtube.com/watch?v=dwlwREGR8sM ↩︎